In December 2025, the World Health Organisation (WHO) issued its first guidance on using Glucagon-Like Peptide 1 (GLP 1) therapies for treating obesity1. The GLP-1 medications covered include liraglutide (Saxenda), semaglutide (Wegovy) and tirzepatide (Mounjaro / Zepbound in the US).
Obesity is a complex chronic disease and a major driver of non-communicable diseases, including cardiovascular disease, type 2 diabetes and several cancers2. Obesity impacts populations across all countries and globally there are approximately 2.1 billion adults who are overweight or have obesity. It is forecast that this will substantially rise to around 3.2 billion by 2050 – accounting for almost 60% of the adult population3.
In their report, two main WHO conditional recommendations are:
-
- GLP-1 therapies may be used for long term obesity treatment in adults (excluding pregnant women).
- Alongside GLP‑1 therapies, structured behavioural interventions—such as healthy eating and increased physical activity—may be offered.
The WHO stresses that obesity cannot be addressed effectively by medications alone. Their conditional recommendations are part of a strategy that includes regular physical activity, healthy diets and support from healthcare professionals. Therefore, three strategic pillars are identified to help combat obesity, in conjunction with GLP-1 therapeutics, namely:
- Strengthen population level policies to create healthier environments.
- Protecting high risk individuals with targeted screening and early interventions.
- Ensuring equitable access to lifelong, person centred care.
The WHO guidance also highlights major challenges including high costs, limited supply and disparities in global access. Even with rapid scale up in production, fewer than 10% of people who could benefit from GLP-1 therapies are expected to have access by 2030.
Countries are being urged to establish fair and affordable routes so those with the greatest medical need are prioritised. The guidance urges global stakeholders to explore strategies such as pooled procurement, tiered pricing and voluntary licensing to expand availability.
Throughout 2026, the WHO aims to collaborate with key stakeholders to develop a fair, transparent and prioritised framework so those with the greatest need receive treatment first.
Introduction
The therapeutic approach to obesity and type 2 diabetes mellitus (T2DM) is evolving in a similar way to how clinicians use antibiotics: targeting several pathways that often produce stronger and more durable effects than acting on a single pathway.

Glucagon-like peptide-1 receptor agonists (GLP-1RAs) laid the foundation, but the complexity of fat mass regulation quickly revealed the limits of one hormonal signal1. This has led to multi-hormonal agents that act simultaneously on glucagon-like peptide-1 (GLP-1), glucose-dependent insulinotropic polypeptide (GIP), glucagon, amylin and/or peptide YY (PYY), better replicating the physiological and coordinated post-prandial response.
By engaging these pathways, the new therapies achieve broader and more synergistic metabolic improvements, marking a shift from single target drugs to integrated hormone-based treatment1.
GLP-1–Based Therapies
GLP-1 is secreted by intestinal endocrine cells after nutrient ingestion. It enhances glucose-dependent insulin secretion, slows gastric emptying, reduces appetite and promotes weight loss1–5. Central nervous system GLP-1 signalling within the hypothalamus and brainstem is central to regulating fat mass6.
Beyond glycaemia, GLP-1 exerts anti-inflammatory, endothelial and lipid-modulating effects1. Long-acting GLP-1RAs on their own such as semaglutide achieve substantial weight loss and glycaemic improvement, aided by gradual dose escalation strategies that improve tolerability1.
Oral semaglutide represents a significant advancement, using SNAC (sodium N-(8-[2-hydroxybenzoyl] amino) caprylate) to overcome gastrointestinal degradation and enable systemic absorption, despite low bioavailability (~1%) and strict fasting administration requirements7.
Further innovations include small-molecule oral GLP-1RAs, such as orforglipron, which activate the GLP-1 receptor (GLP-1R) without peptide structures and offer simpler administration but without the same weight loss range1,8-9.
GIP-Related Therapies
GIP is also released by different endocrine cells in the small intestine. It stimulates insulin secretion during normoglycemia and influences lipid storage, though its metabolic effects are highly context-dependent1.
Importantly, both GIP receptor (GIPR) agonism and GIPR antagonism have been shown to reduce body weight; an unexpected therapeutic paradox1. Central GIPR signalling suppresses appetite in rodents, while peripheral GIP actions vary with insulin sensitivity1,10. In humans, exogenous GIP shows limited appetite loss (anorectic) effects, suggesting species-specific physiological differences11.
GLP-1/GIP Dual Agonists
Dual agonism of the GLP-1R and GIPR aims to capitalise on complementary hormonal effects. Tirzepatide is the first approved dual GLP-1/GIP agonist and achieves greater weight loss and glycaemic improvement than semaglutide alone, suggesting synergistic incretin modulation12. Additional co-agonists, including SCO-094, VK2735, CT-388 and DR10627, are under development to refine receptor balance and broaden metabolic benefits1.
Unimolecular GLP-1RAs/GIPR Antagonists
In contrast to co-agonists, unimolecular agents combining GLP-1R activation with GIPR blockade exploit evidence that GIPR antagonism enhances weight loss by disrupting adipogenic GIP signalling and amplifying GLP-1 driven satiety pathways1.
Maridebart cafraglutide (formerly AMG-133) exemplifies this approach by merging GLP-1 agonism with a monoclonal GIPR-blocking antibody. Monthly dosing produces meaningful body weight reductions (12–16%) and improves glycaemia in people with obesity and T2DM1,13. Pre-clinical work with the GIPR antagonist AT-7687 shows similar synergy when paired with GLP-1RAs1.
Oxyntomodulin Physiology and Oxyntomodulin-Based Therapies
Oxyntomodulin (OXM) is also secreted by the endocrine cells in the intestine but does not have a dedicated receptor. Instead OXM binds to both the glucagon and GLP-1R14. Glucagon as a standalone peptide is secreted by pancreatic alpha-cells. It increases hepatic glycogenolysis and gluconeogenesis during fasting but also regulates satiety, enhances hepatic β-oxidation, reduces liver fat and increases energy expenditure1,15.
OXM mimics many of these same effects when it binds the glucagon receptors14. These metabolic properties support OXM use within multi-agonist therapies, without the risk of pure glucagon’s inherent hyperglycaemic potential.
OXM analogues (GLP-1/Glucagon Co-agonists)
Co-activation of GLP-1R and glucagon receptors leverages the anorectic and insulinotropic actions of GLP-1 with glucagon-driven increases in energy expenditure. Survodutide and mazdutide are leading examples. Survodutide has demonstrated up to 13–15% weight loss, alongside significant improvement in metabolic dysfunction–associated steatohepatitis (MASH)1,16-17. Mazdutide produces dose-dependent weight reduction and glycaemic improvement with good tolerability18.
Triple GIP/GLP-1/Glucagon Co-agonists
Retatrutide is a triple agonist that simultaneously activates GLP-1Rs, GIPRs and glucagon receptors. This design aims to maximise appetite suppression and thermogenesis. In phase 2 trials, retatrutide achieved approximately 17–18% weight loss in individuals with obesity without T2DM, surpassing most available pharmacotherapies1,19.
Amylin Physiology and Amylin-Based Therapies
Amylin is co-secreted with insulin and slows gastric emptying, suppresses glucagon and increases satiety through pathways distinct from other anorectic hormones 1,20. Long-acting analogues such as cagrilintide produce clinically significant weight loss21.
Amylin/GLP-1 Dual Agents
CagriSema, a fixed combination of semaglutide and cagrilintide that integrates GLP-1–mediated appetite suppression with amylin driven satiety and gastric emptying effects. Recent trials show approximately 23% weight loss, exceeding either monotherapy or approaching metabolic surgery efficacy1,21.
Peptide YY Physiology and Related Medicines
Peptide YY (PYY) is co-secreted with GLP-1 by endocrine cells in the intestine and converted to its active form PYY 3-36, which acts via Y2 receptors to inhibit neuropeptide Y (NPY) neurons and promote satiety1,22. After bariatric surgery, postprandial PYY, GLP-1 and OXM rises sharply and contributes to improved adipocyte mass regulation. Early PYY analogues show reduced food intake and modest weight loss in short-term studies1,22.
Table 1. Comparison Table of Novel GLP-1–Based Medications
Conclusion
Together, these advances mark a decisive shift in obesity and T2DM therapeutics from a single pathway modulation toward integrated, multimodal hormone-based interventions.
GLP-1 remains the backbone, but layering complementary signals from GIP, glucagon, amylin and PYY allows for unprecedented degrees of weight reduction and metabolic restoration, as summarised for comparison in Table 1.
As uni-, dual- and triple-molecular agents continue to refine receptor balance, the field is rapidly approaching the efficacy once achievable only through metabolic surgery.
The emerging challenge is no longer whether we can produce profound metabolic benefits, but rather how to optimise durability, individualise receptor targeting and translate these complex pharmacologic innovations into long term clinical decision making.
This therapeutic evolution represents not merely incremental drug development, but a redefinition of how we conceptualise and treat the chronic diseases of obesity and type 2 diabetes.
On October 14th, 2025, the KHNI hosted an expert scientific webinar; “Adapting Appetites: Scientific and Industry Perspectives on the rise of GLP-1 Medications”. The expert panel explored the latest science behind Glucagon Like Peptide-1s (GLP-1s), consumer behaviours across regions, the unique nutritional needs of users and what this means for future innovation in food and beverages.
Latest Scientific Insights on GLP-1s
 Professor Catherine Godson, Professor of Molecular Medicine, University College Dublin (UCD) and Director of the UCD Diabetes Complications Research Centre, began her session discussing the evolution of GLP-1s which were initially indicated for people with type 2 diabetes. Given that GLP-1s result in weight loss, the next approach was to explore if they had a positive effect on people with obesity. Professor Godson highlighted GLP-1 established indications as well as other indications that are under investigation. Interestingly, Catherine pointed out that the incretin hormone GLP-1 not only acts on the cells in the pancreas but also in other areas of the body such as the brain. Professor Godson concluded her session addressing the efficacy, safety, and tolerability of GLP-1s.
Professor Catherine Godson, Professor of Molecular Medicine, University College Dublin (UCD) and Director of the UCD Diabetes Complications Research Centre, began her session discussing the evolution of GLP-1s which were initially indicated for people with type 2 diabetes. Given that GLP-1s result in weight loss, the next approach was to explore if they had a positive effect on people with obesity. Professor Godson highlighted GLP-1 established indications as well as other indications that are under investigation. Interestingly, Catherine pointed out that the incretin hormone GLP-1 not only acts on the cells in the pancreas but also in other areas of the body such as the brain. Professor Godson concluded her session addressing the efficacy, safety, and tolerability of GLP-1s.
Regional Trends in GLP-1 User Behaviour
 Elizabeth Horvath, VP of Marketing for Kerry North America, took us through findings from GLP-1 consumer surveys conducted by Kerry in the US (quantitative survey) and the UK (qualitative survey). The quantitative survey looked at GLP-1 users’ purchase drivers and preferences whereas the qualitative survey explored GLP-1 user habits throughout the entire day to understand their daily activities. Elizabeth highlighted there were five very specific GLP-1 consumers, each on their own health journeys, and that their attitudes and behaviours shift at every stage of the GLP-1 journey. Interestingly, the North America study showed that two-thirds of GLP-1 users are actively seeking functional benefits from their food, beverages, and supplements. Among their top priorities are support for cognitive function, digestive wellness, and immune health. Elizabeth shared insights into how GLP-1 users’ buying habits are changing, especially in foodservice and retail.
Elizabeth Horvath, VP of Marketing for Kerry North America, took us through findings from GLP-1 consumer surveys conducted by Kerry in the US (quantitative survey) and the UK (qualitative survey). The quantitative survey looked at GLP-1 users’ purchase drivers and preferences whereas the qualitative survey explored GLP-1 user habits throughout the entire day to understand their daily activities. Elizabeth highlighted there were five very specific GLP-1 consumers, each on their own health journeys, and that their attitudes and behaviours shift at every stage of the GLP-1 journey. Interestingly, the North America study showed that two-thirds of GLP-1 users are actively seeking functional benefits from their food, beverages, and supplements. Among their top priorities are support for cognitive function, digestive wellness, and immune health. Elizabeth shared insights into how GLP-1 users’ buying habits are changing, especially in foodservice and retail.
Nutrition Essentials for GLP-1 Users
 Next, Angie Jefferson focused on the nutritional needs of GLP-1 users. Initially, Angie introduced the different GLP-1 medications on the market. Currently, there are few good quality trials exploring the impact of GLP-1 medication on consumer eating habits, dietary intakes, and/or their impact on nutritional status. Angie pointed out that a much higher proportion of weight loss in GLP-1 users is attributed to loss of lean body mass; however, GLP-1 use combined with resistance exercise can help preserve or increase muscle mass. Angie provided insights into the nutritional status and emerging needs of GLP-1 users. She also noted that discontinuing GLP-1 treatment often leads to weight regain, with a tendency toward increased body fat percentage. Angie wrapped up by stressing an urgent gap exists in dietary and lifestyle guidance for GLP-1 users.
Next, Angie Jefferson focused on the nutritional needs of GLP-1 users. Initially, Angie introduced the different GLP-1 medications on the market. Currently, there are few good quality trials exploring the impact of GLP-1 medication on consumer eating habits, dietary intakes, and/or their impact on nutritional status. Angie pointed out that a much higher proportion of weight loss in GLP-1 users is attributed to loss of lean body mass; however, GLP-1 use combined with resistance exercise can help preserve or increase muscle mass. Angie provided insights into the nutritional status and emerging needs of GLP-1 users. She also noted that discontinuing GLP-1 treatment often leads to weight regain, with a tendency toward increased body fat percentage. Angie wrapped up by stressing an urgent gap exists in dietary and lifestyle guidance for GLP-1 users.
Innovation Opportunities in Food & Drink for GLP-1 Users
 Dr Alexandra Boelrijk, Kerry VP R&D Proactive Health and Food Protection, looked at opportunities and challenges when considering products for GLP-1 users. Alexandra pointed out that the food and beverage companies early to market with products that meet demands of various GLP-1 users have opportunities to defend share as well as drive growth. Dr Boelrijk highlighted that forward-thinking brands are addressing the needs of GLP-1 users by reformulating products with higher protein, fibre, and micronutrients and/or by developing functional foods that support gut health, satiety, and metabolic support. Alexandra concluded by discussing the new formats of products that have launched in the market for GLP-1 users.
Dr Alexandra Boelrijk, Kerry VP R&D Proactive Health and Food Protection, looked at opportunities and challenges when considering products for GLP-1 users. Alexandra pointed out that the food and beverage companies early to market with products that meet demands of various GLP-1 users have opportunities to defend share as well as drive growth. Dr Boelrijk highlighted that forward-thinking brands are addressing the needs of GLP-1 users by reformulating products with higher protein, fibre, and micronutrients and/or by developing functional foods that support gut health, satiety, and metabolic support. Alexandra concluded by discussing the new formats of products that have launched in the market for GLP-1 users.

During the Q&A session, moderator Mark Faherty posed thoughtful questions to the speakers. He concluded the webinar by expressing gratitude to Angie, Alexandra, Catherine, and Elizabeth for sharing their time and expertise.
This is a very interesting article that was first posted in June 2025, and due to its popularity the KHNI would like to draw your attention to this informative read.
Over the past decade, the global prevalence of obesity has escalated to alarming levels, prompting significant public health concerns. In 2022, approximately 1 in 8 individuals worldwide were living with obesity (including 1 in 3 in the EU and in North America), with adult obesity rates more than doubling since 1990 and adolescent obesity quadrupling during the same period.
This is particularly pertinent because obesity is a risk factor for many serious diseases and disorders such as cardiovascular diseases and type 2 diabetes which are major contributors to premature deaths. The WHO acceleration plan to stop obesity has outlined strategies for governments to address this issue, including introducing nutrition labelling schemes that support consumers to make healthier choices, as well as monitoring the food environment for nutritional quality, prices and marketing practices.
Front-of-Pack Nutrition Labelling: A Decade of Global Transformation
Many governments globally have introduced front of pack (FOP) nutrition labelling and regulations around sugar, fat, and salt as a key lever to combat obesity and associated non-communicable diseases. FOP nutrition labelling can empower consumers to make healthier food choices by simplifying the nutritional information into clear visual cues, using colour, ratings or symbols, making it easier to compare products.
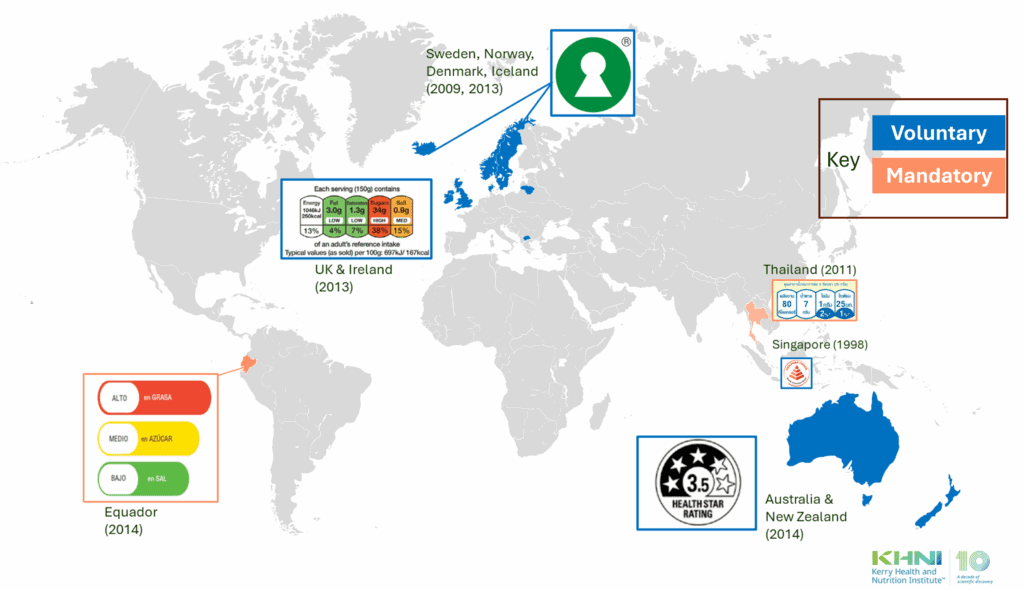
Figure 1 shows the countries who were early adopters of FOP nutritional labelling. As early as 1989, Sweden added the voluntary ‘Keyhole symbol’ to their food labels, which was then added by Norway & Demark in 2009, followed by Iceland & Lithuania in 2013, and Macedonia in 2015. Other European countries included a voluntary nutrition traffic light label in 2013 (UK & Ireland), while a similar mandatory label was implemented in Ecuador in 2014. Australia and New Zealand also implemented a voluntary label known as the “Health Star” system in 2014.
Figure 1: Front-of-Pack Nutrition Labelling prior to 2015
Since 2015, various countries have implemented or proposed even more FOP nutrition labelling systems to provide accessible, at-a-glance nutritional information. Figure 2, highlights the evolution of FOP nutrition labelling globally as of 2025.
Figure 2: Front-of-Pack Nutrition Labelling 2025
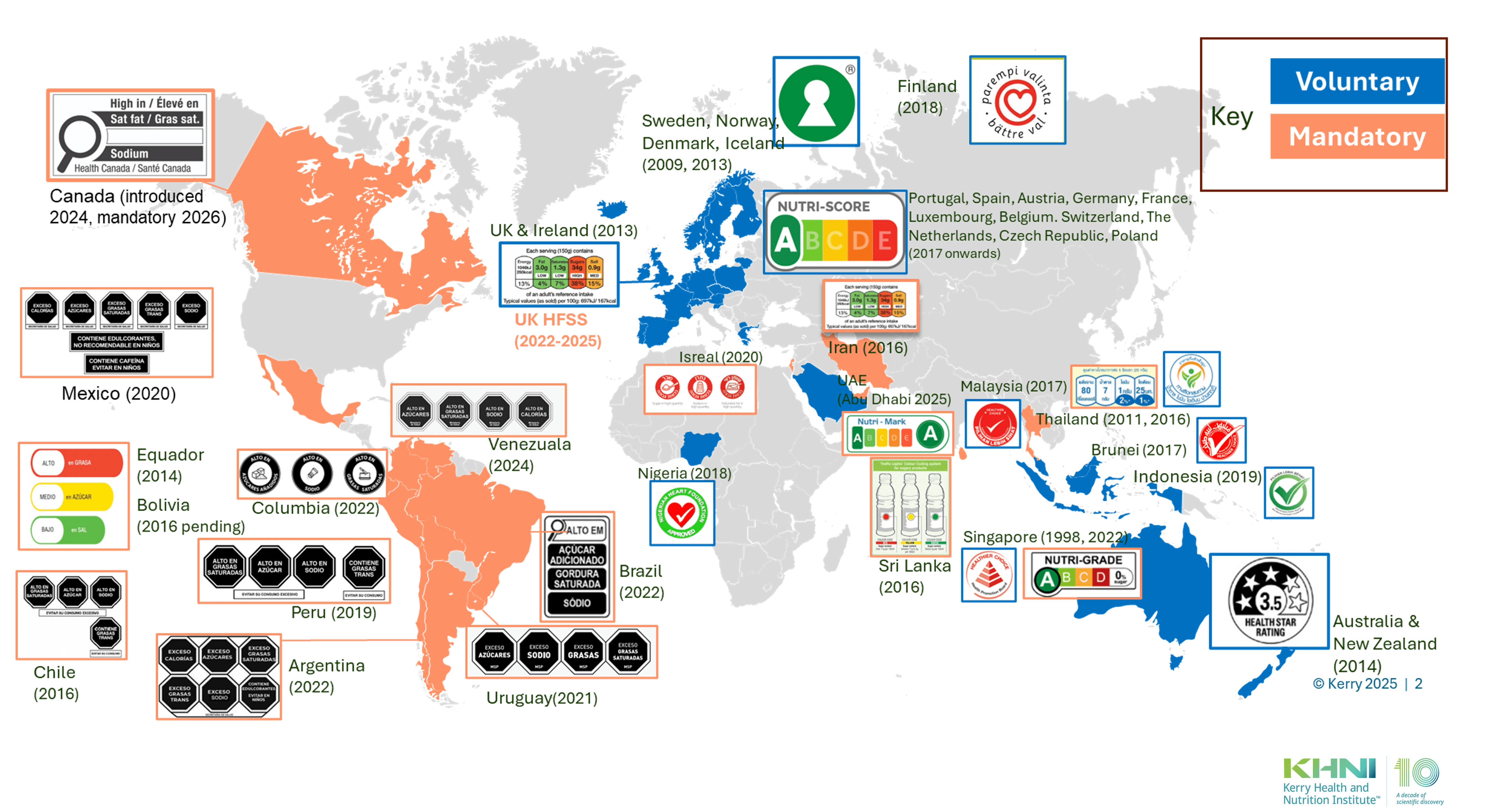
Notable Changes in FOP Nutrition Labelling since 2015:
-
- European Union: Several EU countries have adopted the Nutri-Score system, a voluntary FOP nutrition labelling scheme that rates the nutritional quality of food products using a color-coded scale from A (healthiest) to E (least healthy). France implemented Nutri-Score in 2017, followed by Belgium, Spain, Germany, and others.
- Latin America: In 2016, Chile implemented black octagonal warning labels on foods high in calories, sugar, sodium, or saturated fat. This measure led to a significant reduction in the purchase of unhealthy items and prompted food manufacturers to reformulate products to avoid the warning labels. Since this implementation, several Latin American countries have also adopted similar labelling (Peru in 2019; Mexico in 2020; Uruguay in 2021; Argentina, Brazil and Colombia in 2022; and Venezuela in 2024), with some differences between countries, but all of them mandatory.
- Canada: Health Canada introduced mandatory FOP nutrition label in 2022, with full implementation required by January 1, 2026. The label highlights products high in saturated fat, sugars, and sodium, aiming to assist consumers in making informed choices.
- South East Asia: Many countries in South East Asia have introduced healthier choice logo’s. In 2022 Singapore introduced the mandatory Nutri-Grade label and advertising restrictions for all pre-packaged beverages, and out of home beverages from fountain dispensers, automated coffee machines and cafe’s / food service premises. The Nutri-Grade system rates beverages according to their sugar and saturated fat levels, with a special sugar declaration mark for toppings added.
- United Kingdom: In addition to the voluntary FOP traffic light label for pre-packaged foods, the UK has implemented mandatory regulations to reduce advertising of foods and drinks high in fat, salt, and sugar (HFSS) to combat childhood obesity. These regulations, effective October 1, 2025, include a ban on HFSS ads on TV before 9 PM and a complete ban on paid-for online ads for these products. The regulations, as outlined in the Advertising (Less Healthy Food Definitions and Exemptions) Regulations 2024, are designed to limit exposure of children to HFSS products through advertising.
- Middle East: Colour coded traffic light labels have been introduced for pre-packaged foods in Iran (mandatory), the Kingdom of Saudi Arabia, and the United Arab Emirates (voluntary).
- Sugar Taxes on sugar sweetened beverages: Globally over 100 countries have introduced levies on pre-packaged sugar sweetened beverages to promote healthier beverage choices by consumers.

Future Considerations for FOP Nutrition Labelling
-
- Singapore: From mid-2027, the Nutri-Grade labelling requirements and advertising prohibitions will be extended to key contributors of sodium and saturated fat intake. These measures will apply to 23 sub-categories of prepacked salt, sauces, seasonings, instant noodles, and cooking oils (SSSIO) sold in retail settings.
- China has started to encourage companies to actively adopt the recommended standards of “Guidelines on graphic symbol of front-of-pack nutrition labelling in pre-packaged Food” , which introduced four front-of-pack nutrition labels simultaneously depending on products’ nutritional profile, including a black-and-white warning label, an A-D rating, and a “Smart Choice” message.
- India: FSSAI engaged with the Indian Institute of Management (IIM) to seek expert advice on the most consumer-friendly front-of-pack labelling (FOPL) system used globally. IIM conducted an in-depth survey to assess consumer preferences for various nutrition labels in India. The results indicated that the Health Star Rating (HSR) system was the most preferred, owing to its ease of identification, understanding, reliability, and influence on consumer choices. Based on these findings, in February 2022 FSSAI decided to adopt the Indian Nutrition Rating (INR), a modified version of Australia’s HSR, tailored to suit Indian consumer behaviour and dietary patterns.
- USA: On January 14, 2025, the Food and Drug Administration (FDA) issued the long-awaited Proposed Rule on Front-of-Package (FOP) Nutrition Labelling. The Nutrition Info box will categorize the levels of saturated fat, sodium, and added sugars as “Low,” “Med,” or “High,” making it easier for consumers to understand the nutritional content at a glance. There are also plans to remove certain foods and beverages HFSS from SNAP (supplemental nutrition assistance program) US.
While these initiatives have shown promise in influencing consumer behaviour and encouraging product reformulation, their impact will be determined by regulatory framework, industry acceptance, and market restrictions. For FOP nutrition labelling to be fully beneficial it must be paired with broader public health policies that address the needs of healthy and sustainable dietary habits, such as education, accessibility, and cultural needs. As obesity rates continue to rise globally, the adoption and refinement of FOP nutrition labelling remain critical components of public health strategies.
Disclaimer: This article is based on information available as of June 12, 2025.