Vitamin A is more frequently associated with vision but it plays multiple roles in supporting the immune system, including:
-
- maintaining the integrity of skin and mucosal barriers that protect from pathogen invasion.
- supporting the innate (general) immune system (e.g. regulating Natural Killer (NK) cell production, supporting phagocytic activity of macrophages).
- supporting the adaptive (specialised) immune system (e.g. development and differentiation of Th1 and Th2 cells which direct the destruction of invading cells, B cell mediated antibody responses to antigen) 1, 2.
There is an approved European Commission health claim for vitamin A, stating that it “contributes to the normal function of the immune system”, and is available to foods that meet defined criteria within the EU 3.
Recommended Intakes
Vitamin A recommendations for adults vary by region:
-
- China: the Chinese Nutrition Society Reference Nutrient intake (RNI) is 660mg per day for adult women and 770mg per day for adult men up to 50 years 4.
- Europe: the European Food Safety Authority (EFSA) population reference daily intakes (PRI) are 650 micrograms for women and 750 micrograms for men 5.
- United States: the Institute of Medicine (IOM) recommended dietary allowance (RDA) is 700 micrograms per day for women and 900 micrograms per day for men 6.
Dietary Sources
Vitamin A in the diet comes from two sources: preformed vitamin A (retinol and retinyl esters) and provitamin A (carotenoids). Preformed vitamin A is found in foods from animal sources, while provitamin A are plant pigments that include beta-carotene, alpha-carotene, and beta-cryptoxanthin. These provitamin A carotenoids are converted into vitamin A in the body, although conversion efficiency shows considerable variation and is influenced by the food source, an individual’s vitamin A levels, and the amount eaten 7.
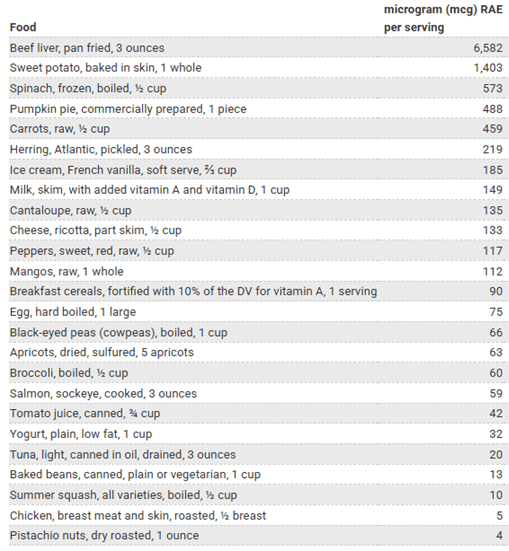
 Preformed Vitamin A or retinol is found in animal products mainly including liver, fish and eggs while provitamin A sources are generally found in colourful vegetables like carrots, sweet potato and peppers (See Table 1).
Preformed Vitamin A or retinol is found in animal products mainly including liver, fish and eggs while provitamin A sources are generally found in colourful vegetables like carrots, sweet potato and peppers (See Table 1).
Some countries such as the US routinely add vitamin A to milk and margarine while some ready-to-eat cereals are also voluntarily fortified with vitamin A. For this reason, it is important to use local information when calculating dietary intakes.
In Western diets, retinol accounts for nearly 65% of total vitamin A intake with carotenoids making up 35% of the total 8 but the contribution of carotenoids is higher in countries such as Southeast Asia and Africa where it can make up to 80% of the vitamin A intake 9. Recent data shows that in China, vegetables are the greatest contributor to total vitamin A intakes 10.
Table 1. Food sources of Dietary Vitamin A 7
Deficiency
Vitamin A deficiency is a public health problem in more than half of all countries especially those in Africa and South-East Asia 11. The most severe effects of vitamin A deficiency are seen in young children and pregnant women in low-income countries, ranging from preventable blindness to a weakened ability to fight infections. Vitamin A deficiency is a double‑edged cycle in which illnesses like diarrhoea and measles further deplete vitamin A levels in the body.
In areas of deficiency, routine vitamin A supplementation is recommended in infants and children up to 5 years of age 12. Other strategies include dietary based approaches, biofortification, and food fortification. Even in developed countries, the importance of vitamin A in the very young is recognised, e.g. it is recommended that children in the UK aged 6 months to 5 years take a vitamin supplement containing vitamins A, C and D every day 13.
Excess Intakes
As vitamin A is fat-soluble, it can be stored in the body, particularly the liver and excessive intakes can cause harm. The US IOM set an upper limit of 3,000mg per day of pre-formed vitamin A for adult men and women including pregnant adults 4. The EFSA have set the same upper limit for adults including women of child-bearing age, pregnant and lactating women and post-menopausal women. Lower limits are recommended for younger groups 14.
In terms of the provitamin, beta-carotene, there is no indication that intakes from dietary sources are linked to adverse health effects. However, smokers have been recommended to avoid consuming food supplements containing beta-carotene, and their use by the general population should be limited to the purpose of meeting vitamin A requirements 14.
Vitamin A Supplementation
 Vitamin A deficiency affects not only the growth and development of children but also increases susceptibility to infectious diseases including respiratory and gastrointestinal infections 8.
Vitamin A deficiency affects not only the growth and development of children but also increases susceptibility to infectious diseases including respiratory and gastrointestinal infections 8.
Across Asia, India and Africa, vitamin A supplementation has been associated with a lower incidence of diarrhoea and measles among children (low quality evidence) while all-cause mortality was also reduced with supplementation (high quality evidence) 15.
A 2024 Cochrane review showed that vitamin A supplementation did not prevent or reduce the duration of acute upper respiratory infections (URTIs) in children up to seven years of age in low to middle income countries 16. However, this was based on a limited number of studies and more research is needed.
Contributor:
Kerry Health and Nutrition Institute
![]() We bring the voice of science to some of the most challenging questions facing the food and beverage industry day to day through our network of over 1000 Kerry scientists, external collaborators, and our Scientific Advisory Council.
We bring the voice of science to some of the most challenging questions facing the food and beverage industry day to day through our network of over 1000 Kerry scientists, external collaborators, and our Scientific Advisory Council.
-
References
- Gombart AF, Pierre A, Maggini S. (2020) A Review of Micronutrients and the Immune System-Working in Harmony to Reduce the Risk of Infection. Nutrients 12: 236. DOI: 10.3390/nu12010236
- Ross AC. (2012) Vitamin A and retinoic acid in T cell-related immunity. Am J Clin Nutr 96: 1166S–72S. DOI: 10.3945/ajcn.112.034637
- EU Commission. (2012) Commission Regulation (EU) No 432/2012 establishing a list of permitted health claims made on foods, other than those referring to the reduction of disease risk and to children’s development and health. Last accessed March 16, 2026.
- Institute of Medicine. (2001) US Panel on Micronutrients. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. Last accessed March 16, 2026.
- EFSA (2015) NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies). Scientific opinion on Dietary Reference Values for vitamin A. EFSA J 13:4028, 84. DOI: 2903/j.efsa.2015.40
- Chinese Nutrition Society. (2023) Dietary Reference Intakes for China (2023) – A Summary Report. Last accessed March 16, 2026.
- National Institutes of Health. (2025) Vitamin A and Carotenoids Fact Sheet for Health Professionals. Last accessed March 16, 2026.
- Weber D, Grune T. (2012) The contribution of β-carotene to vitamin A supply of humans. Mol Nutr Food Res 56: 251–258. DOI: 10.1002/mnfr.201100230.
- FAO/WHO. (1998) Joint FAO/WHO Expert Consultation on Human Vitamin and Mineral Requirements. Vitamin and mineral requirements in human nutrition: report of a joint FAO/WHO expert consultation, Bangkok, Thailand. Last accessed March 16, 2026.
- Li X, Guo C, Zhang Y, et al. (2023) Contribution of Different Food Types to Vitamin A Intake in the Chinese Diet. Nutrients 15: 4028. DOI: 10.3390/nu15184028
- Hu Q, Lyu J, Li J, et al. (2025) A comprehensive analysis of vitamin a deficiency burden and trends: insights from the global burden of disease study 2021 and future predictions to 2050. Front Nutr 12: 1673576. DOI: 10.3389/fnut.2025.1673576
- WHO. (2011) Guideline: Vitamin A supplementation in infants and children 6–59 months of age. Geneva, World Health Organization. Last accessed March 16, 2026.
- NHS. (2024) Vitamins for children. Last accessed March 16, 2026.
- EFSA Panel on Nutrition, Novel Foods and Food Allergens (NDA); Turck D, Bohn T, Castenmiller J, et al. Scientific opinion on the tolerable upper intake level for preformed vitamin A and β-carotene. EFSA J 22: e8814. DOI: 10.2903/j.efsa.2024.8814
- Imdad A, Mayo-Wilson E, Haykal MR, et al. (2022) Vitamin A supplementation for preventing morbidity and mortality in children from six months to five years of age. Cochrane Database Sys Rev 3: CD008524. DOI: 10.1002/14651858.CD008524.pub4
- Cheng X, Li D, Yang C, et al. (2024) Oral vitamin A supplements to prevent acute upper respiratory tract infections in children up to seven years of age. Cochrane Database Sys Rev 5: CD015306. DOI: 10.1002/14651858.CD015306.pub2