Nutrition is inherently multidisciplinary, drawing from the physical sciences, medicine, public health, psychology, sociology, and increasingly, planetary health 1. Therefore, nutrition science research is essential for advancing our understanding of human health and supporting evidence based decision making. Research in this space aims to clarify how nutrients, bioactives, and other food components influence health, inform dietary guidance and policy, and support strategies to prevent disease.
A wide range of study designs are used in nutrition research, and no single study design can answer every question 2. Understanding the purpose, strengths, and limitations of each approach helps distinguish between stronger and weaker evidence, so the hierarchy of research methods is key to evaluating the quality of evidence.
This article outlines the key study designs used in nutrition research, the types of questions they are best suited to answer, and the strengths and limitations that guide how their findings should be interpreted, based on several resources 1-5.
Visualising study designs as a pyramid (Figure 1) highlights how evidence strength varies. Studies at the lower levels of the pyramid tend to offer limited, less practical insights, while those at the top delivering stronger evidence with greater relevance to real world nutrition choices 3,4.
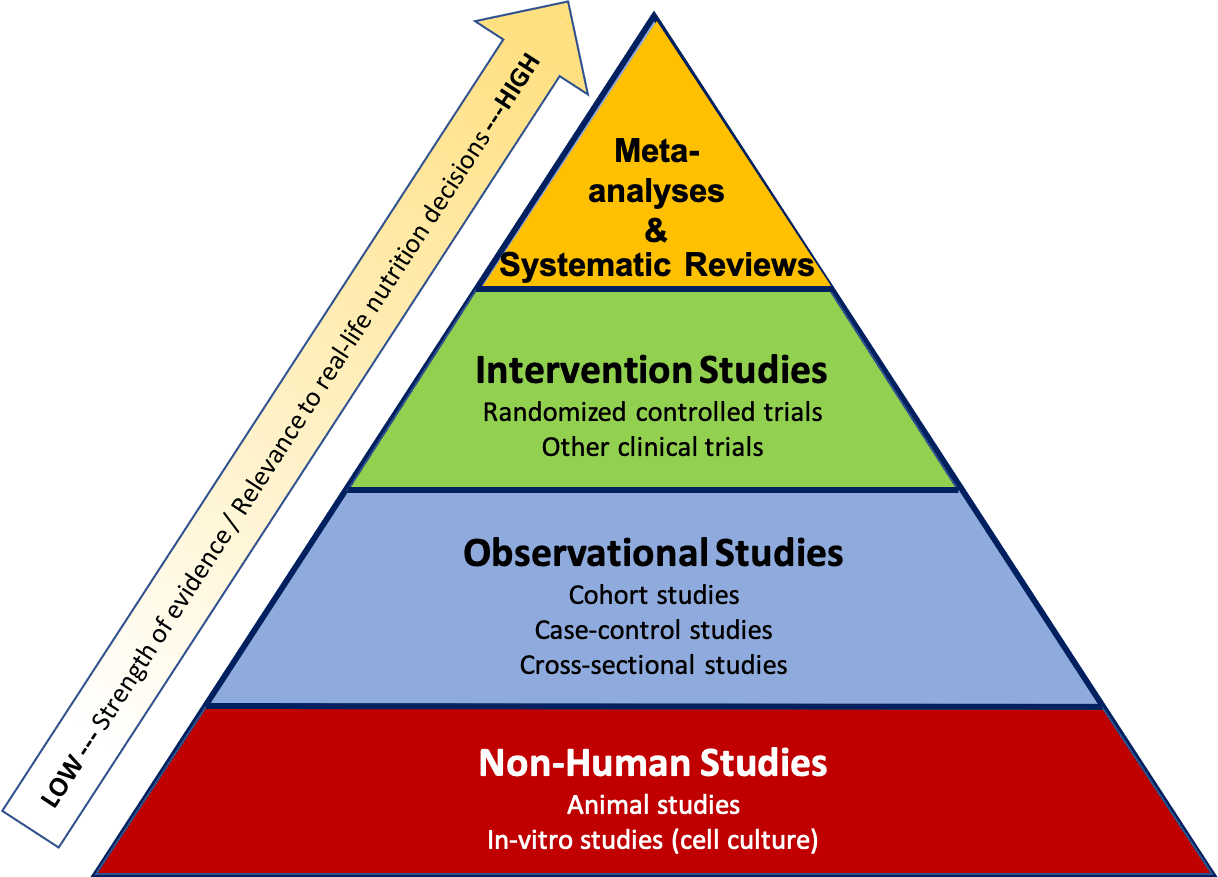
Figure 1. The hierarchy of evidence ranks different types of research according to the strength of the conclusions 3. (Licensed under CC BY 4.0)
Systematic reviews and meta analyses sit at the top of this hierarchy because they provide data across multiple studies to provide more comprehensive conclusions. Randomised controlled trials and prospective cohort studies typically provide the most robust evidence when examining relationships between dietary exposures and health outcomes. However, the rapid growth of the field — and the diversity of methods used — can make it challenging for practitioners and consumers to interpret findings and translate them into practice.
Foundational Research: Non-Human Studies
Foundational research — including in vitro studies in cells or tissues and in vivo studies in animal models — plays a critical role in uncovering the biological mechanisms that underpin how nutrients, ingredients, and other food components behave in controlled settings. These early stage studies provide directional evidence that helps shape hypotheses and supports the rationale for human research.

It is important to note that isolated cells and tissues and animals do not replicate the complexity of human physiology. Differences in metabolism, exposure levels, and biological responses mean that findings cannot be directly translated to human outcomes. For instance, a compound that influences cellular metabolism in vitro, for example, may behave very differently within the interconnected systems of the human body.
However, the value of foundational research becomes clear when it is integrated with human data. For example, while observational research links smoking with cancer, cell studies identify the carcinogenic compounds responsible. So, when mechanistic evidence aligns with human outcomes, confidence in the overall conclusion(s) is strengthened.
Observational Studies
These studies track large groups of people over time, in real-world settings, to understand how lifestyle behaviours — including dietary patterns — relate to health outcomes. These studies identify population level patterns and provide potential associations that may warrant further investigation in more controlled study designs. Observational studies cannot determine cause and effect relationships and, hence, the impact of a single dietary or lifestyle factor.
Common observational designs include prospective cohort studies, case–control studies, and cross sectional studies, each offering different strengths for understanding how diet and lifestyle influence long term health.
Case Control Studies
Case control studies compare people who already have a specific health condition (the cases) with similar individuals who do not (the controls). Researchers then look back in time to assess whether past exposures — such as dietary habits — differ between the two groups. For example, comparing fruit and vegetable intake in people with and without heart disease may help identify potential associations with disease risk.
These studies are relatively quick and cost effective, making them especially useful for investigating rare conditions or outcomes that would be difficult to study prospectively. They can also examine multiple potential risk factors at once and often serve as an important first step in identifying associations that warrant further research.
However, case control studies face several methodological challenges. Because exposure information is collected retrospectively, they are highly susceptible to recall bias — particularly when individuals with a disease remember past behaviours differently from those without it. Selection bias, confounding, and reverse causation can also limit the strength of conclusions. For instance, if higher consumption of non sugar sweeteners is observed among people with obesity, it may reflect dietary changes made after weight gain rather than a causal effect of sweeteners.
Cohort Studies
Cohort studies are observational studies that are either prospective or retrospective, depending on when the data were collected. In a prospective cohort, participants complete questionnaires and undergo measurements at the start of the study. On the other hand, with retrospective cohort studies, researchers “look back” to analyse the relationship.
Prospective cohort studies follow large groups of people in real world conditions over many years — sometimes decades — to explore how dietary and lifestyle exposures relate to the development of diseases. Participants provide information at baseline and at regular intervals on factors such as diet, physical activity, and health status. Dietary intake is usually self reported, which introduces challenges such as misreporting, difficulty estimating portion sizes, and changes in behaviour over time.
By tracking outcomes over time, researchers can examine patterns and test hypotheses. Collectively, prospective cohort studies have shaped much of our understanding of how diet and lifestyle influence chronic disease risk, such as cardiovascular disease or osteoporosis. However, their long duration means they are time and resource intensive. As with all observational research, these studies can identify associations but cannot establish cause and effect relationships.
Cross Sectional Studies
This type of research provides a snapshot of health behaviours, exposures, and outcomes in a population at a single point in time. They are typically conducted through surveys or brief assessments that collect information on both potential risk factors and health indicators simultaneously.
However, cross sectional research has important limitations. Because exposure and outcome are measured at the same moment, it is not possible to determine which came first. This raises the issue of reverse causality — for example, whether a dietary behaviour contributes to a health outcome or whether the health outcome influences how participants report their diet. Cross sectional studies can also be affected by selection bias and recall bias, particularly when participants’ awareness of their health status shapes how they report past behaviours.
Despite these constraints, cross sectional studies are cost effective, relatively quick to conduct, and useful for estimating the prevalence of dietary habits, lifestyle behaviours, or health conditions in a population. They can also highlight potential associations worth exploring in more rigorous study designs. A typical cross sectional study might compare dietary patterns across countries to explore whether differences in diet align with variations in cardiovascular disease prevalence.
Randomised Controlled Trials (RCTs)
Randomised controlled trials (RCTs) are considered the gold standard for determining cause and effect relationships 1,2,5. Participants are recruited and randomly assigned to a control (placebo) group or an intervention group, ensuring the groups are comparable at baseline. For example, in an RCT examining the Mediterranean diet and cardiovascular risk, the control group might follow a standard low fat diet while the intervention group adopts a Mediterranean pattern 3. After a defined study period, researchers compare outcomes such as heart attacks or strokes between groups. Because randomisation minimises confounding factors, differences in outcomes can be attributed to the intervention itself. This is why RCTs provide the strongest evidence for causation rather than correlation. When conducted as double blind trials, neither participants nor researchers know who receives the treatment, further reducing bias and mitigating placebo effects.
Despite their strengths, RCTs come with practical and ethical constraints. They are expensive, often involve small sample sizes, and may struggle with long term adherence, especially when testing complex dietary patterns. Ethical considerations limit the ability to test harmful exposures or withhold beneficial treatments.
Systematic Reviews and Meta Analyses
Systematic reviews and meta analyses sit at the top of the evidence hierarchy because they provide a comprehensive overview of existing evidence and can reveal whether findings are consistent across different populations and settings. However, these methods are only as strong as the quality and consistency of the studies they include, and ensuring relevant studies are not missed or intentionally excluded.
However, these methods are only as robust as the quality and consistency of the studies they include, and they rely on thorough, unbiased inclusion of all relevant evidence.
A systematic review uses a structured, transparent process to identify, evaluate, and summarise all relevant research on a specific question. When the included studies are sufficiently similar in design, population, and outcomes, researchers may conduct a meta analysis, which statistically pools results to generate a single, weighted estimate of effect. Larger, well designed studies contribute more heavily to this estimate than smaller or lower quality studies.
Systematic reviews and meta analyses help determine whether scientific findings are consistent, generalisable, and reliable, and they often guide policy decisions, clinical recommendations, and future research priorities.
In Summary
Science is a continuous process. It can move slowly and often involves uncertainty, yet it remains the most reliable way to build understanding about the world and human health. Many types of studies contribute to this evidence base, each with its own strengths and limitations, and no single study provides a definitive answer. Progress happens because researchers continually evaluate and refine one another’s work, identifying opportunities to improve methods and explore new questions.
Contributor:
Aisling Aherne, PhD RNutr FAfN FIFST CSci
Senior Nutrition Scientist
 Aisling has over 25 years of experience working in nutritional science including scientific research, clinical nutrition, science communications, and nutritional science & regulations. Her current role involves regularly adding content to the KHNI website as well as organising KHNI webinars. Additionally, Aisling will continually look for opportunities where the KHNI can participate at external events.
Aisling has over 25 years of experience working in nutritional science including scientific research, clinical nutrition, science communications, and nutritional science & regulations. Her current role involves regularly adding content to the KHNI website as well as organising KHNI webinars. Additionally, Aisling will continually look for opportunities where the KHNI can participate at external events.
-
References
-
- Martyn K. (2025) Understanding nutrition research for better patient care. BMJ Nutr Prev Health 8: e001241. doi: 10.1136/bmjnph-2025-001241.
- EUFIC (2023) The levels of evidence in nutrition research.
- Lane Community College’s Nutrition: Science and Everyday Application (2026) “Types of Research and How to Interpret Them” CC BY-NC 4.0
- Tufts University Libraries (2026) Interpreting Nutrition Evidence.
- Harvard School of Public Health. (2025) Research Study Types. The Nutrition Resource.
-
