Globally, there are approximately 2.1 billion adults who currently are overweight or have obesity. It is forecast that this will substantially rise to around 3.2 billion by 2050 – accounting for almost 60% of the adult population 1. This highlights that traditional approaches to curbing the prevalence of overweight and obesity have had limited success. Immediate and effective interventions are clearly needed to address the overweight and obesity public health crisis.
In recent years, pharmacological interventions have emerged as important adjuncts to traditional weight loss approaches. These obesity medications, such as Glucagon Like Peptide-1 Receptor Agonists (GLP-1 RAs), have gained significant attention for their promising efficacy in achieving weight loss. Currently, there are several GLP-1 RA medications delivered by injection, which are sold under various brand names, though availability and licensing vary significantly by country (Table 1).
Table 1. Examples of Global Usage of GLP-1 RAs for Weight Management
GLP-1 RAs are prescription-only pharmaceutical drugs and not dietary supplements. They must be prescribed and monitored by a qualified healthcare professional. Furthermore, it must be emphasised that holistic treatment strategies including lifestyle and dietary changes should be included alongside GLP-1 RAs medications.
Unsurprisingly, where data is available, GLP-1 RA usage continues to accelerate, particularly with the forthcoming release of an oral form, which will likely make medications lower cost and more widely accessible. Additionally, usage is likely to further increase given upcoming expiring patents from 2026 onwards 9,10, enabling the provision of more widespread, lower cost formulations.
It is estimated that in the US, over 90 million adults are eligible for GLP-1 RAs, with approximately 26 million adults eligible in the UK. In the US, individuals with overweight or obesity using GLP-1 RAs has increased from 21,000 in 2019 to 174,000 in 2023, which is a 700% increase in usage 11. In Australia in 2023, there were approximately 2.5 million prescriptions for Semaglutide alone under the Pharmaceutical Benefits Scheme, which is nearly double the previous year’s total prescription 12. However, globally, real usage is likely higher given the difficulties accurately quantifying usage due to the burgeoning private market.
While North America held the largest market share for GLP-1 RA medications in 2024, with Europe following, Asia-Pacific is expected to exhibit the fastest growth market due to rising diabetes and obesity rates 13. Although the Middle East and Africa market is currently smaller, it is also projected to grow significantly in the coming years 14. GLP-1 RAs face a mix of regulatory hurdles across Latin America, shaped by fragmented healthcare systems, evolving drug policies, and rising demand. Yet, the Latin American GLP-1 RA market is expected to grow by a third in the next five years 15.
Understanding the Biological Effects of GLP-1 RAs
GLP-1 RAs, also known as GLP1-analogs or incretin mimetics, are a class of obesity medications originally developed for the management of type 2 diabetes. They mimic the action of endogenous GLP-1, a hormone naturally released by cells in the small intestine in response to food intake and exert effects 16 (Figure 1) in a dose-dependent manner 17. Figure 1. Physiological Effects of GLP-1 RAs.
Figure 1. Physiological Effects of GLP-1 RAs.
Primarily, GLP-1 RAs help regulate blood glucose levels by stimulating insulin secretion from pancreatic beta cells, whilst decreasing the production of glucagon, a hormone that increases blood glucose. Additionally, GLP-1 RAs modulate the hypothalamus (the region in the brain that controls appetite) to regulate hunger, slow gastric emptying, and regulate gut hormones such as leptin (a hormone that helps regulate body weight on a long-term basis). Consequently, this prolongs the feeling of fullness (satiety), reduces appetite, and reduces overall calorie intake – subsequently leading to negative energy balance and weight loss 18.
Efficacy of GLP-1 RAs in Weight Loss
GLP-1 RAs have consistently demonstrated effectiveness for weight loss in clinical trials among individuals with obesity compared with placebo treatments 17,18. Those using GLP-1 RAs achieve clinically meaningful weight loss of between 5 to 24% of their initial body weight, depending on dosing regime and type of drug administered. Furthermore, reductions in the incidence of cardiovascular events have also been evidenced 19.
GLP-1 RA Side Effects and Adherence
Despite the promising efficacy of GLP-1 RAs for weight loss, dropout rates in clinical trials and adherence concerns in real-world settings are notable. Real‐world studies demonstrate high discontinuation rates of GLP‐1RAs by up to 75% within the first year of use, predominantly driven by side effects 20-22. Common side effects include gastrointestinal symptoms such as nausea, vomiting, diarrhoea, and constipation. Other side effects may include headaches, dizziness, fatigue, and injection site reactions. Rare, but potentially serious, side effects of GLP-1 RAs may include pancreatitis and gallbladder disease, as highlighted by The UK Medicines and Healthcare Products Regulatory Agency in 2024 23.
Whilst GLP-1 RA usage is effective at driving weight loss, the magnitude varies depending on factors such as the type of GLP-1 RA used, treatment duration, and the individual. Weight regain following discontinuation of these medications is common (Figure 2), with up to two-thirds of weight loss being regained within the first year 24. This is likely driven by the lack of education surrounding lifestyle and behaviour change strategies adopted by GLP-1 RA users, which would encourage continued healthy lifestyle habits following medication cessation.
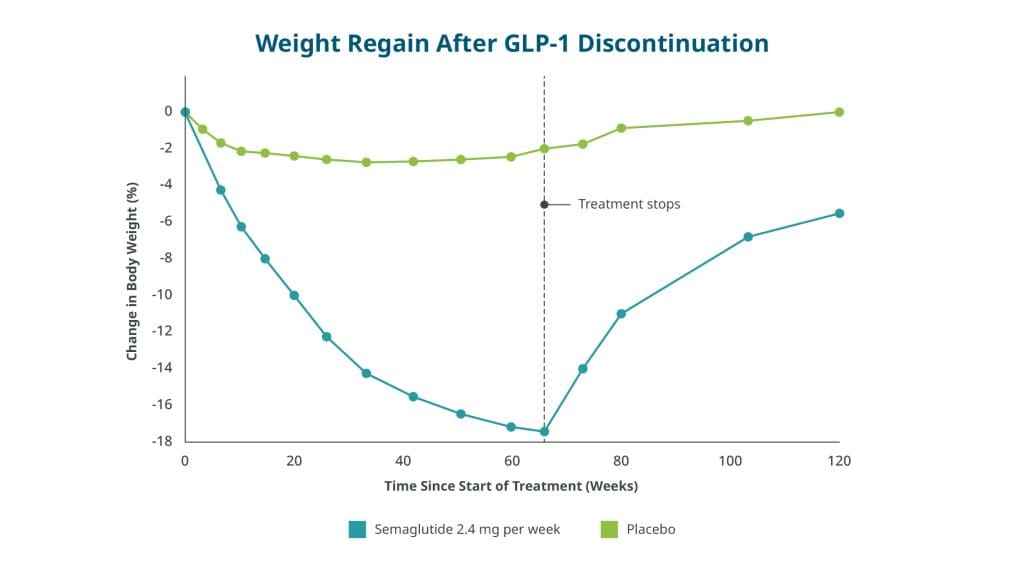
Figure 2. Weight Regain After GLP-1 RA Discontinuation 24. Reproduced from Wilding et al. 24, © [2022], published by Wiley, under CC-BY license.
Dietary Intakes of GLP-1 RA Users – what is scientific evidence telling us?
Most of the general population fall short of achieving a healthy, balanced diet. For example, many populations are not meeting the recommendations for fibre intake including those in Argentina, Canada, China, Lithuania, South Africa, the UK, and US. Further, from national and international dietary survey data across the globe, sugar, saturated fat and sodium intakes remain above recommended levels. Consequently, achieving a nutritionally adequate, balanced diet may be particularly challenging for GLP-1 RA users, who consume a reduced proportion of their usual daily intake, unless careful attention is given to food choices.
A narrative review of 10 primary studies that assessed energy intakes in GLP-1 RA users revealed that total calorie intake was reduced by 16 to 39% in a single meal 25. However, the most common measurement of food intake was a standardized test meal followed by an ad libitum lunch, dinner, or snack. This method has inherent limitations and data should be treated with caution. Only one study included in the review used a validated 24-h dietary recall method. Interestingly, when data is studied in more detail, reported calorie intake remains adequate and in line with recommendations for GLP-1 RA users. For example, reported daily energy intake of GLP1-RA users is approximately 1750 to 2180 kcal per day. So perhaps meeting recommended nutrient intakes remains achievable.
Beyond changes in calorie intake, only eight studies, to date, have evaluated changes in macronutrient intake in GLP-1 RA users. Unfortunately, data is inconsistent among these studies, likely due to the different methodologies used between studies, making it difficult to provide firm conclusions. Perhaps more concerning is that 11 to 50% of total weight loss in GLP-1 RA users is attributed to loss of lean body mass, which may detrimentally include loss of skeletal muscle 26, potentially negatively impacting metabolism, strength and long-term health. Thus, protein intake, alongside physical activity, remains a priority to minimise muscle loss for GLP-1 users.
GLP-1 RA Recommendations
In studies evaluating combined GLP-1 RA with nutrition and lifestyle interventions, individuals receiving both GLP-1 RAs and structured dietary guidance achieved greater weight loss, better adherence, and were more likely to sustain weight loss after discontinuing GLP-1 RAs compared to those receiving the medication alone 27.
Although limited information currently exists regarding specific dietary reference intakes for individuals using obesity medications, a recent Joint Advisory highlights specific areas of nutritional concern for GLP-1 users (Figure 3) 27. For example, protein intakes of up to 1.5 g/kg/day have been suggested for this population 28. Yet, in practice, these protein levels are likely difficult to achieve in a population of GLP-1 RA users who have 1) a higher body mass and 2) a reduced energy intake. Future protein intake recommendations should be based on lean mass-adjusted body weight rather than total body weight, as protein requirements are largely determined by lean tissue rather than fat mass.

Figure 3. Key elements of nutritional priorities to support GLP-1 therapy users for obesity 27. Reproduced from Mozaffarian et al. 27, © [2025], published by Wiley, under CC-BY license.
For Healthcare Professionals (HCPs)
Tailored approaches to GLP-1 RA treatment plans are needed to ensure sustainable weight loss strategies, improve patient adherence, and support healthier dietary intakes. Previous research has recommended nutritional priorities to support GLP-1 RA users (Figure 3). These recommendations can enable healthcare professionals (HCPs) to better guide GLP-1 RA users toward lasting health improvements. For example, HCPs should discuss the importance of balanced nutritional intake with all patients prescribed GLP-1 RAs, alongside monitoring signs of malnutrition, micronutrient status, and changes in body composition.
Given the limitations in accurately quantifying body composition using more accessible body compositional measurement tools (e.g., bioelectrical impedance), physical function should also be monitored. Further, to promote sustained weight management, GLP-1 RA users should be educated on healthy diets and physical activity recommendations, and support should be available to encourage long term behaviour change.
For Researchers
There is a clear need for future research to examine changes in dietary intake and nutrient status following use of obesity medications using robust study designs with validated, accurate methods for measuring daily habitual intakes. Given that, to our knowledge, only two studies have estimated micronutrient intake in GLP-1 RA users 29,30, more research is needed to both quantify changes in micronutrient intake and status in this population.
Further, whilst some anecdotal and qualitative data suggests that GLP-1 RAs effectively reduced food-related thoughts (‘food noise’) and support healthier eating behaviours, more objective data is needed. Mechanistically, more research is needed to investigate whether GLP-1 RAs influence nutrient absorption and subsequent bioavailability, incorporating measurements of the gut microbiota diversity and composition, and nutrient biomarkers.
Such research will help develop nutritional guidance to best support GLP-1 RA users. Information available on dietary reference intakes for individuals using obesity medications is minimal 28, and currently not well-evidenced.
An Industry Perspective on Innovating for GLP-1 Users
The surge in GLP-1 RA usage for weight loss is set to increase demand for products with a wide range of attributes. Portion size, protein and fibre content, and digestive health are the key areas for consideration.
There are a few strategic approaches that are currently gaining momentum across the food, beverage and supplement industries 31 (Figure 4). One strategy is to position existing products as complementary solutions for GLP-1 RA users. Focusing on gut health aids that might alleviate gastrointestinal side effects and nutritional supplements that help offset deficiencies linked to reduced food intake. Another approach is to launch products that are nutrient-dense and portion-controlled for both GLP-1 RA users and individuals tapering off the medication who continue to sustain weight loss whilst preserving muscle mass.
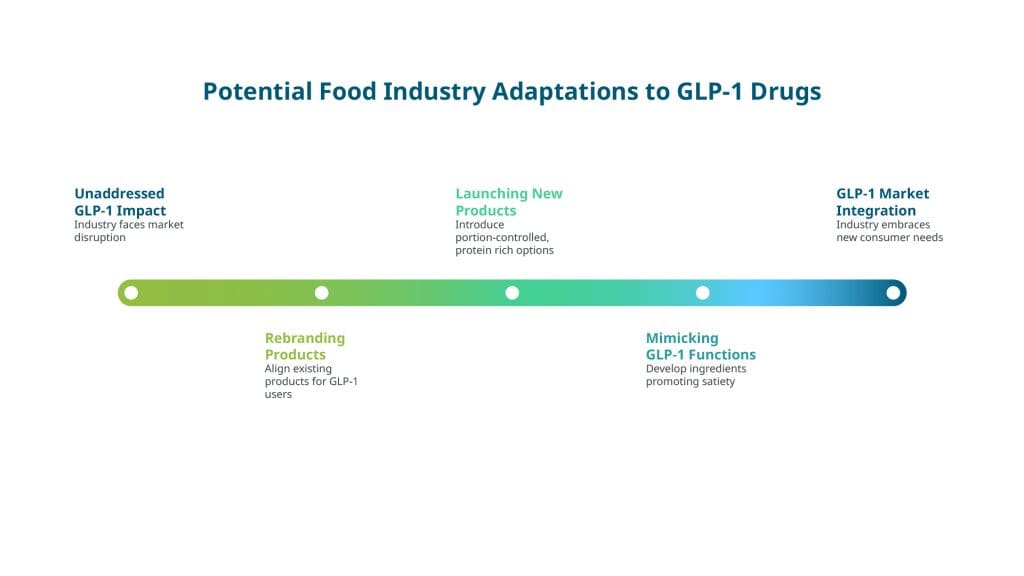 Figure 4. GLP-1 RA Strategic Approaches for Industry 31.
Figure 4. GLP-1 RA Strategic Approaches for Industry 31.
In Summary
GLP-1 RAs represent a valuable therapeutic option to achieve weight loss and improve overall health when prescribed safely and appropriately alongside dietary and behavioural support and increased physical activity.
By balancing the potential benefits and risks of treatment using evidence-based strategies, HCPs are well placed to help optimise the use of GLP-1 RAs in the management of obesity and overweight. This will ultimately support individuals in achieving their weight loss goals while minimising adverse effects.
Research is still required to evidence nutritional intake in GLP-1 RA users, and to subsequently inform dietary recommendations that are specific for this population. Nutritious products must be accessible to GLP-1 users to achieve healthy eating habits that provide essential nutrients, vitamins, and minerals.
Authors’ Note: The authors recognize the fast-evolving nature of GLP-1 research and trends and will endeavour to ensure the article remains current with emerging GLP-1 RA data.