This article is part of a mini-series on Women’s Health, exploring the unique health requirements and needs of women throughout their life stages. To read Part I: The Hormone Lifecycle Journey, click here.
Whether it’s preparing for a family, going through pregnancy, or breastfeeding, motherhood is a transformative time in a woman’s life. Such an intricate journey is filled with moments of anticipation, joy, and connection. But it can also include challenges and health considerations that require thoughtful attention and care. The link between a mother’s health and their infant’s wellbeing has created a strong consumer demand for products targeting conception, pregnancy, and breastfeeding. Of recent launches in the Women’s Supplements Market, 38% were related to pregnancy and/or fertility 1.
The fertility stage is oftentimes the gateway to family living. Around 186 million individuals live with infertility worldwide, at times leading to feelings of guilt, fear, and self-blame 2. Support, whether from healthcare professionals, family, and/or friends, is key to helping people navigate the complexities of the fertility journey with dignity, resilience, and hope.
Polycystic Ovary Syndrome (PCOS)
Polycystic Ovary Syndrome (PCOS) affects an estimated 6 – 13% of women, with up to 70% of cases being undiagnosed. Around 40% of all female fertility disorders are due to ovulatory disorders 3, with 85% of these linked to PCOS 4. Considering PCOS causes one in three cases of female infertility and affects 6 – 13% of women of reproductive age, there’s demand for naturally derived, science-backed solutions to help promote fertility for those living with PCOS 5.
The mechanism behind infertility associated with PCOS is one that is still being explored due to the number of factors that can contribute to this condition.
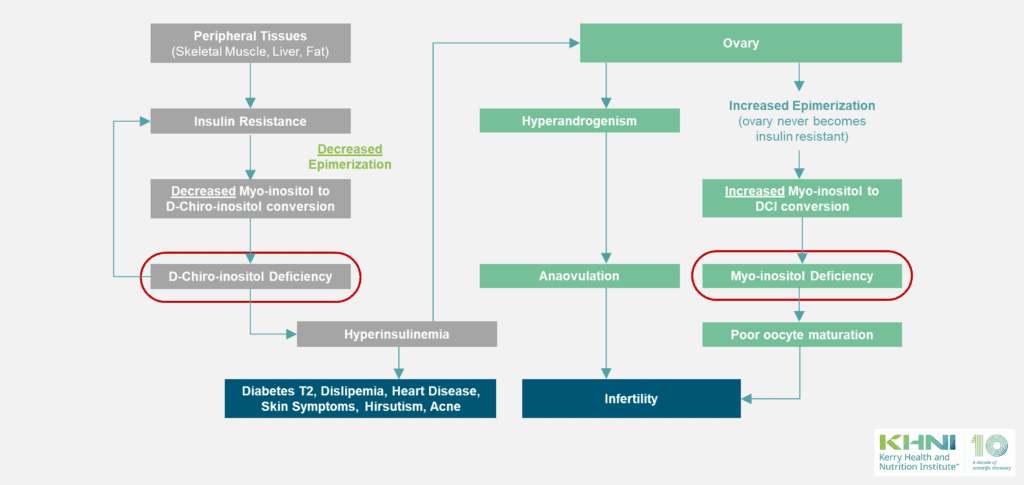
However, it is evident from the research that one of the main factors that impact this condition is insulin resistance. This insulin resistance has a direct effect on Myo-inositol (MI) to D-Chiro-Inositol (DCI) conversion, ultimately causing a DCI deficiency. This deficiency can lead to hyperinsulinemia, i.e., high levels of insulin, which can cause an overstimulation of the ovary to produce testosterone. i.e., hyperandrogenism, which in turn causes anovulation. In parallel to this, there is a MI deficiency in the ovary which leads to poor oocyte maturation. This is because MI is involved oocyte maturation. This together with anovulation can contribute to infertility associated with PCOS.
Biosynthesis of myoinositol (MI) occurs endogenously, primarily in the kidney, with a rate approaching 4g per day. The conversion rate of MI to D-chiro-inositol (DCI) ranges from 3% to about 9% 6. In women suffering PCOS, they have a systemic deficiency of DCI 7,8. Consequently, the level of DCI in tissues can decrease significantly. On the contrary, the situation seems to be different in the ovary, where there is a deficiency of MI 9. Therefore, women experiencing PCOS have DCI deficiency at a systemic level and MI deficiency at the ovary level.
To tackle both deficiencies, varying combinations of MI and DCI have been researched. For instance, a ratio 40:1 MI:DCI taken by healthy women resulted in better clinical results that the use of MI or DCI alone 10,11. Interestingly, a clinical trial comparing the benefits of a MI:DCI ratio at 3.6:1 versus ratio 40:1 showed significantly better results in the MI:DCI 3.6:1 group with almost four times more live births than the 40:1 MI:DCI group 12. Furthermore, a MI:DCI 3.6:1 ratio has multi-dimensional benefits to women with PCOS such as regularizing menstrual cycles and improving insulin resistance, hormonal, glycaemic, and lipid profiles, with considerable efficacy and tolerability 12-15.
Pregnancy
Pregnancy is a time of incredible change for women as their bodies prepare to nurture a new life. A mother’s health becomes paramount as her well-being and that of her baby is intricately connected. Emotional health is equally important during this time, as hormonal changes bring about a variety of feelings, from joy and excitement to anxiety and mood swings. A strong support network is crucial to help expecting mothers navigate the changes and challenges with strength and confidence.

A well-balanced diet of good quality carbohydrates, proteins, specific fatty acids, vitamins and minerals is essential to support changes to the mother’s body and for optimal growth and development of the baby 16. It is also important that mothers are aware of the foods that must be avoided during pregnancy including unpasteurized dairy foods, soft cheeses, raw meat and fish, and alcohol 16. Mothers’ diets have also been found to influence a baby’s health into adulthood, with good prenatal nutrition reducing the risk of heart disease, diabetes and high blood pressure in adulthood.
Interestingly, a study reported that up to 92% of pregnant women reported taking prenatal vitamins and/or other supplements 17. Some of the most popular supplements are folic acid, which is essential for preventing neural tube defects in the developing foetus, and Docosahexaenoic acid (DHA), which is key for cognitive, eye and heart development. Omega-3 DHA fatty acids are critical for the development of the baby’s brain and eyes, reduces the risk of preterm birth, supports maternal health, and contributes to healthy birth weight.
Breastfeeding
From conception to their second birthday, babies’ first 1,000 days of life are a critical window for good nutrition and infant wellbeing. During this time, a baby’s gut and immune system develop rapidly as they move from a protected environment to one exposed to many immune challenges.

Breastfeeding is a journey that fosters a unique bond between mother and baby. Regarded as the gold standard of infant nutrition, it offers a host of extraordinary benefits for both mother and baby. A nutrient-rich diet and good hydration is vital for breastfeeding mothers, especially for those who are exclusively breastfeeding as they generally need an extra 300 – 500kcal per day 16.
However, it is important to understand that every mother’s situation is unique, and breastfeeding comes with its own challenges, which means it isn’t always possible. Acknowledging these challenges openly helps to create a more supportive environment that equips mothers with the tools they need to best care for themselves and their babies.
One of the main medical reasons for women stopping breastfeeding is mastitis. According to the World Health Organisation (WHO), up to 30% of lactating women suffer from mastitis 18. Through extensive research, intake of a probiotic strain isolated from woman breastmilk, Lactobacillus fermentum CECT 5716, promoted breast health and comfort. This, in turn, prevented premature cessation of breastfeeding due to pain, by reducing mastitis pain symptoms and the incidence or recurrence of mastitis 19-21.
Summary
Addressing fertility and health challenges for women requires a multifaceted approach that includes dietary and lifestyle modifications. Emerging research underscores the powerful role of nutrition in managing the key drivers of PCOS. Incorporating nutrient-rich foods, maintaining a balanced macronutrient intake, and adopting sustainable dietary patterns can empower women to improve their fertility outcomes. As science continues to advance, personalized nutrition strategies show promise for tailoring solutions to individual needs, offering hope for those navigating fertility challenges. Supporting women on this journey is not just about dietary choices; it’s about fostering overall health and well-being for the future.
Contributors:
Mónica Olivares Martín, PhD
RD&A Director, Women & Infant Health - Kerry
 Mónica graduated in Pharmacy from the University of Granada in Spain and did her doctoral thesis on molecular biology at a Research Center of the Spanish National Research Council (CSIC). She specializes in probiotic strains isolated from human milk and is the author of 80 scientific publications, more than 40 related to probiotics, and is also listed as an inventor on 8 patents, 3 of them on probiotics.
Mónica graduated in Pharmacy from the University of Granada in Spain and did her doctoral thesis on molecular biology at a Research Center of the Spanish National Research Council (CSIC). She specializes in probiotic strains isolated from human milk and is the author of 80 scientific publications, more than 40 related to probiotics, and is also listed as an inventor on 8 patents, 3 of them on probiotics.
Mollie Mulligan, MSc ANutr
Marketing Executive - Kerry
 Mollie is an Assistant Marketing Manager in Cognitive Health on Kerry’s Global ProActive Health team. She holds an MSc in Insight & Innovation from Dublin City University, a BSc in Human Nutrition from University College Dublin and is a Registered Associate Nutritionist (ANutr).
Mollie is an Assistant Marketing Manager in Cognitive Health on Kerry’s Global ProActive Health team. She holds an MSc in Insight & Innovation from Dublin City University, a BSc in Human Nutrition from University College Dublin and is a Registered Associate Nutritionist (ANutr).
-
References
- Innova Database Search, 2025
- Ombelet W. (2020) WHO fact sheet on infertility gives hope to millions of infertile couples worldwide. Facts Views Vis Obgyn. 12 (4): 249-251. PMCID: PMC7863696.
- WHO (2024) Infertility – Factsheet. Available at: https://www.who.int/news-room/fact-sheets/detail/infertility. (Last accessed: 07 July 2025)
- Ombelet W, Cooke I, Dyer S, et al. (2008) Infertility and the provision of infertility medical services in developing countries. Hum Reprod Update14 (6): 605-21. doi: 10.1093/humupd/dmn042.
- WHO (2025) Polycystic ovary syndrome – Factsheet. Available at: https://www.who.int/news-room/fact-sheets/detail/polycystic-ovary-syndrome (Last accessed: 07 July 2025)
- Bizzarri M, Monti N, Piombarolo A, et al. (2023) Myo-Inositol and D-Chiro-Inositol as Modulators of Ovary Steroidogenesis: A Narrative Review. Nutrients 15 (8): 1875-1889. doi: 10.3390/nu15081875.
- Baillargeon JP, Diamanti-Kandarakis E, Ostlund RE Jr, et al. (2006) Altered D-Chiro-Inositol Urinary Clearance in Women With Polycystic Ovary Syndrome. Diabetes Care 29 (2): 300-5. doi: 10.2337/diacare.29.02.06.dc05-1070.
- Lentini G, Querqui A, Monti N, Bizzarri M. (2025) PCOS and Inositols – Advances and Lessons We are Learning. A Narrative Review. Drug Des Devel Ther. 9: 4183-4199. doi: 10.2147/DDDT.S524718.
- Heimark D, McAllister J, Larner J. (2014) Decreased myo-inositol to chiro-inositol (M/C) ratios and increased M/C epimerase activity in PCOS theca cells demonstrate increased insulin sensitivity compared to controls. Endocr J. 61 (2): 111-7. doi: 10.1507/endocrj.ej13-0423.
- Lete I, Martínez A, Lasaga I, et al. (2024). Update on the combination of myo-inositol/d-chiro-inositol for the treatment of polycystic ovary syndrome. Gynecol Endocrinol. 40 (1). http://DOI: 10.1080/09513590.2023.2301554.
- Nordio M, Proietti E. (2012) The combined therapy with myo-inositol and D-chiro-inositol reduces the risk of metabolic disease in PCOS overweight patients compared to myo-inositol supplementation alone. Eur Rev Med Pharmacol Sci. 16 (5): 575-81. http://PMID: 22774396.
- Mendoza N, Diaz-Ropero MP, Aragon M, et al. (2019) Comparison of the effect of two combinations of myo-inositol and D-chiro-inositol in women with polycystic ovary syndrome undergoing ICSI: a randomized controlled trial. Gynecol Endocrinol. 35 (8): 695-700. doi: 10.1080/09513590.2019.1576620.
- Mendoza N, Galan MI, Molina C, et al. (2020) High dose of d-chiro-inositol improves oocyte quality in women with polycystic ovary syndrome undergoing ICSI: a randomized controlled trial. Gynecol Endocrinol. 36 (5): 398-401. doi: 10.1080/09513590.2019.1681959.
- Kachhawa G, Senthil Kumar KV, Kulshrestha V, et al. (2022) Efficacy of myo-inositol and d-chiro-inositol combination on menstrual cycle regulation and improving insulin resistance in young women with polycystic ovary syndrome: A randomized open-label study . Int J Gynaecol Obstet. 158 (2): 278-284. doi: 10.1080/09513590.2019.1681959
- Vyas L, Raiturker AP, Sud S, et al. (2022) Management of polycystic ovary syndrome among Indian women using myo-inositol and D-chiro-inositol. Bioinformation18 (2): 103-110. doi: 10.6026/97320630018103.
- British Nutrition Foundation (2025) Diet in Pregnancy: A Review of Current Challenges and Recommendations. A British Nutrition Foundation Briefing Paper. Nutrition Bulletin
- Dou JF, Middleton LYM, Zhu Y, et al. (2022) Prenatal vitamin intake in first month of pregnancy and DNA methylation in cord blood and placenta in two prospective cohorts. Epigenetics & Chromatin 15, 28 (2022). doi 10.1186/s13072-022-00460-9
- Inch S, von Xylander S. (2020) Mastitis Causes and Management (2000) Available at: http://apps.who.int/iris/bitstream/10665/66230/1/WHO_FCH_CAH_00.13_eng.pd. (Last accessed: 07 July 2025)
- Arroyo R, Martín V, Maldonado A, et al. (2010) Treatment of infectious mastitis during lactation: antibiotics versus oral administration of Lactobacilli isolated from breast milk. Clin Infect Dis. 50 (12): 1551-8. doi: 10.1086/652763.
- Maldonado-Lobón JA, Díaz-López MA, Carputo R, et al. (2015) Lactobacillus fermentum CECT 5716 Reduces Staphylococcus Load in the Breastmilk of Lactating Mothers Suffering Breast Pain: A Randomized Controlled Trial. Breastfeed Med. 10 (9): 425-32. doi: 10.1089/bfm.2015.0070.
- Hurtado JA, Maldonado-Lobón JA, Díaz-Ropero MP, et al. (2017) Oral Administration to Nursing Women of Lactobacillus fermentum CECT5716 Prevents Lactational Mastitis Development: A Randomized Controlled Trial. Breastfeed Med. 12 (4): 202–9. doi: 10.1089/bfm.2016.0173.