From hidden vulnerabilities to future-ready solutions – our second Kerry Health and Nutrition Institute podcast puts the resilience of today’s food system under the spotlight and asks what it will take to strengthen it.
Hosted by the KHNI and moderated by Mary Shelman, founder of the Shelman Group, this session brought together Wolfram Schlenker, the Ray A. Goldberg Professor of the Global Food System at Harvard University, and Juan Aguiriano, Group Head of Marketing and Sustainability at Kerry.
The discussion examined how climate shocks, environmental pressures, and geopolitical volatility are exposing real fragility – driving all-round disruption leading to unpredictability, supply instability, and price variability.
The panel explored the growing complexity shaping food and agriculture and why resilience must sit at the centre of every decision. Embedding sustainable resilience into risk management was identified as strengthening a company’s ability to forecast and anticipate disruption and ultimately generate long‑term value.
Speakers highlighted the complexities around trade-offs between sustainability, affordability, resilience, and nutrition – while at the same time meeting consumer expectations. They pointed to the expanding role of data and AI in enabling more resilient production systems, smarter and more adaptive supply chains, and better-informed consumer decision-making.
The message is clear: sustainable resilience is no longer a cost – it’s core to risk management and long-term growth. Food’s future lies not in producing more, but in producing better — driven by partnership, innovation, and a mindset built for resilience.

The immune system is constantly active and needs energy from macronutrients like carbohydrates, fats and proteins. Protein also supplies amino acids to build immune cells and enzymes that help destroy pathogens. These enzymes also require vitamins and minerals as cofactors to function properly.
So, while it may sound obvious, a varied and balanced diet that provides adequate nutrients is the foundation of a healthy immune system. However, some nutrients receive particular attention for their role in immune health, including vitamins A, C and D, as well as the minerals such as zinc and selenium1. There is also evidence for the immune benefits of other nutrients and ingredients, such as long-chain omega-3 fatty acids, probiotics and beta-glucans2.
Immunonutrition
Read how each of the nutrients listed below support the immune system. It is important to bear in mind that micronutrients have additional health benefits to immune health. Click on each nutrient/non-nutrient below to learn more:

How the Immune System Works?
The immune system is the body’s way of protecting itself from infection by foreign invaders like bacteria and viruses. It helps the body stay healthy and recover when illness does occur and is made up of the innate (general) and adaptive (specialised) immune system3.
The innate immune system is the body’s first line of defence. When pathogens like infectious bacteria or viruses get into the respiratory tract or gastrointestinal system, the innate immune system responds by sending cells like neutrophils or macrophages to remove the threat. These cells try to engulf the invading pathogen or create enzymes to destroy it.
The adaptive immune system specifically targets the pathogen and takes over from the innate immune system. It is often described as the ‘memory’ of the immune system. Once exposed to a pathogen, the immune system can remember the identity of that pathogen for the future and quickly mount a defence specific to that pathogen.
Impact of Age and Physical Activity on Immune Health

Immune health becomes especially important in vulnerable age groups like infants and the elderly. Both physical and psychological stress can also compromise the immune system. Examples include over-exercising, emotional stress and surgery.
This article was published in March 2022 and updated on June 15, 2026.
On 30 April 2026, the Kerry Health & Nutrition Institute (KHNI) hosted an expert scientific webinar on Megatrends Shaping Tomorrow’s Food. The panel featured the KHNI Scientific Advisory Council: Professor Imed Gallouzi, Dr Lisa Ryan and Professor Martin Bloem.
A central theme was longevity—defined not simply as living longer, but as enabling people to remain cognitively sharp, physically active and independent throughout extended lifespans. The panel highlighted key nutrients that contribute to healthy aging, and that approaches to longevity differ significantly across socio‑economic groups, influencing both affordability and access to nutritious foods. Therefore, equitable longevity solutions must consider these disparities.
With the rapid rise of GLP‑1 medications, the panel discussed both their benefits and emerging concerns. The panel outlined nutrients and food formats that may be particularly supportive for GLP‑1 users. This led to a broader conversation about food processing. While often viewed negatively, processed foods remain a practical necessity and an essential source of nutrition for many populations.
The panel also examined how AI and emerging technologies—such as wearables and smart health systems—are reshaping personalised nutrition. These tools may help individuals monitor stress, understand their nutritional needs and tailor dietary choices to their lifestyles. However, the speakers stressed that the value of these tools depends entirely on the quality, accuracy and representativeness of the data that underpins them. As technology accelerates, ensuring robust, high‑quality data will be critical for delivering meaningful health outcomes.
To close the webinar, just before the Q&A session, each member of the Scientific Advisory Council shared a final take‑home message for the audience. Professor Martin Bloem emphasised the importance of simplicity—whether in health or nutrition, consumers need straightforward practical solutions to help them stay healthy. Dr Lisa Ryan highlighted that optimal health relies on both good nutrition and regular physical activity. Professor Imed Gallouzi underscored the potential of technology, noting that emerging tools can support better eating habits, healthier routines and improved overall lifestyle.
What is the Role of Zinc in Immune Health?
Zinc is a popular nutrient in winter supplements. It is an essential nutrient and the second most abundant trace element in the body, after iron1. It is found in every cell in the body and involved in many bodily processes. It is required by cells from both the innate (general) and adaptive (specialised) immune system2.
The innate immune system is the body’s first line of defence. When pathogens like infectious bacteria or viruses get into the respiratory tract or gastrointestinal system, the innate immune system responds by sending cells like neutrophils or macrophages to remove the threat. These cells try to engulf the invading pathogen or create enzymes to destroy it.
The adaptive immune system specifically targets the pathogen and takes over from the innate immune system. It is often described as the ‘memory’ of our immune system. Once exposed to a pathogen, the immune system can remember the identity of that pathogen for the future and quickly mount a defence specific to that pathogen.
 The role of Zinc in the immune system includes:
The role of Zinc in the immune system includes:
-
- helping to maintain the integrity of the skin and muscular membranes, preventing pathogen entry into the body.
- supporting the growth and differentiation of immune cells.
- supporting the phagocytic activity of monocytes and help regulate cytokine release.
- antibody production, particularly IgG and helping the immune system distinguish between “self” and “non-self”3.
This role has been recognised in an approved European Union health claim for zinc stating that it “contributes to the normal function of the immune system” and is available to foods that meet defined criteria within the EU4.
Are there Recommended Intakes for Zinc?
Zinc recommendations range from 5 to 11mg per day for adults, varying by each global region5. In the US, the Institute of Medicine (IOM) recommendations are 11mg per day for men and 8mg per day for women6. Similarly, the Chinese Nutrition Society Reference intake (RNI) is 12mg per day for adult men and 8.5 mg per day for women8. In Europe, the European Food Safety Authority has established a Population Reference Intake of 9.4 to 16.3mg per day for men with low to higher intakes of dietary phytate and 7.5 to 12.7mg per day for adults women with low to higher intakes of phytate7.
Most people in developed countries get enough zinc through their diet, meaning their immune system isn’t missing the zinc it needs. For example, in the US around 18% of people do not meet the Estimated Average Requirement (EAR) of zinc per day. This means most people are not zinc deficient, but certain people may still benefit from eating more zinc in their diet.
Where can Zinc be Sourced in Dietary Sources
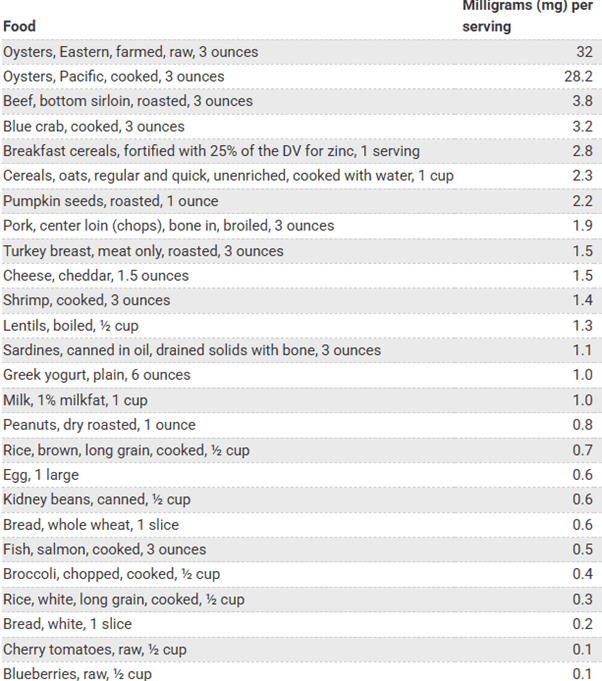
Zinc is mostly found in seafood, beef, poultry, beans, nuts or fortified cereal. Phytic acid, found in cereals, legumes and nuts, is known to decrease zinc bioavailability1. Evidence shows that the biofortification of varieties of staple crops may be useful in improving the zinc status of an individual5.
Table 1. Zinc content of common foods in the diet9
What Happens with a Zinc Deficiency?
Zinc deficiency is a widespread global health issue, particularly prevalent in low- and middle-income countries. About 17.3% of the world’s population10 is at risk of inadequate zinc intake. When the body doesn’t have enough zinc, it does not develop a strong immune response. Zinc deficiency affects many different organs and tissues in the body with signs and symptoms varying by age9. For example, zinc deficiency can delay growth and cause diarrhoea and alopecia in children and it can alter cognitive and psychological function in older adults.
Most people in developed countries get enough zinc through their diet but it can affect more vulnerable groups. For example, the percentage of people in the US that do not meet the Estimated Average Requirement (EAR) of zinc varies from 16% in households with full food security to 27% in those with very low food security11. In Europe, the average intake of zinc is above the recommended amount. However, certain vulnerable populations may benefit from including more zinc rich foods or supplements in their diet e.g. those on plant-based diets with little animal foods and the elderly5.
Are there Health Risk of Excess Intakes?
Excessive amounts of zinc can cause nausea, dizziness, headaches, gastric distress, vomiting and loss of appetite and chronic large doses of 50mg of zinc or more can inhibit copper absorption and reduce immune function9. Excessive intakes from food sources are unlikely but may occur with excessive supplementation. The IOM Tolerable Upper Intake Level for zinc is 40mg per day for adults. EFSA has set the Tolerable Upper Intake Level (UL) for total daily zinc intake from all sources (diet and supplements) at 25mg per day for adults. This level is based on the reduction of copper status12. Lower limits are recommended for younger groups.
Is Zinc Supplementation Effective?
 A 2024 Cochrane review 13 based on 34 randomised controlled trials in children and adults (15 prevention, 19 treatment) showed that compared with placebo, taking zinc preventatively may make little to no difference to whether a person catches a cold or to the duration or severity of the cold. Taking zinc for treatment of an existing cold may reduce the duration but the authors were not confident of the quality of the result which they describe as low to very low.
A 2024 Cochrane review 13 based on 34 randomised controlled trials in children and adults (15 prevention, 19 treatment) showed that compared with placebo, taking zinc preventatively may make little to no difference to whether a person catches a cold or to the duration or severity of the cold. Taking zinc for treatment of an existing cold may reduce the duration but the authors were not confident of the quality of the result which they describe as low to very low.
The most common negative sides effects were irregularities in taste and stomach upset. A recent review however supports a preventive role of zinc supplementation in reducing the incidence and burden of respiratory infections, particularly in children with recurrent disease and in zinc-deficient populations14.
This article was published in March 2020 and updated on March 31, 2026.
What is the Role of Vitamin D in Human Health?
Vitamin D, sometimes known as ‘the sunshine vitamin’, is a fat-soluble vitamin important for bone health, muscle function and the immune system1-4. Vitamin D is also being investigated for its role in protecting against some chronic diseases including cardiovascular disease and type-2 diabetes1.
Vitamin D exists in two primary forms:
- vitamin D2 (ergocalciferol) which is obtained from plant and fungi sources that have been exposed to UV light.
- vitamin D3 (cholecalciferol), found in animal-based products such as fatty fish, eggs and liver3.
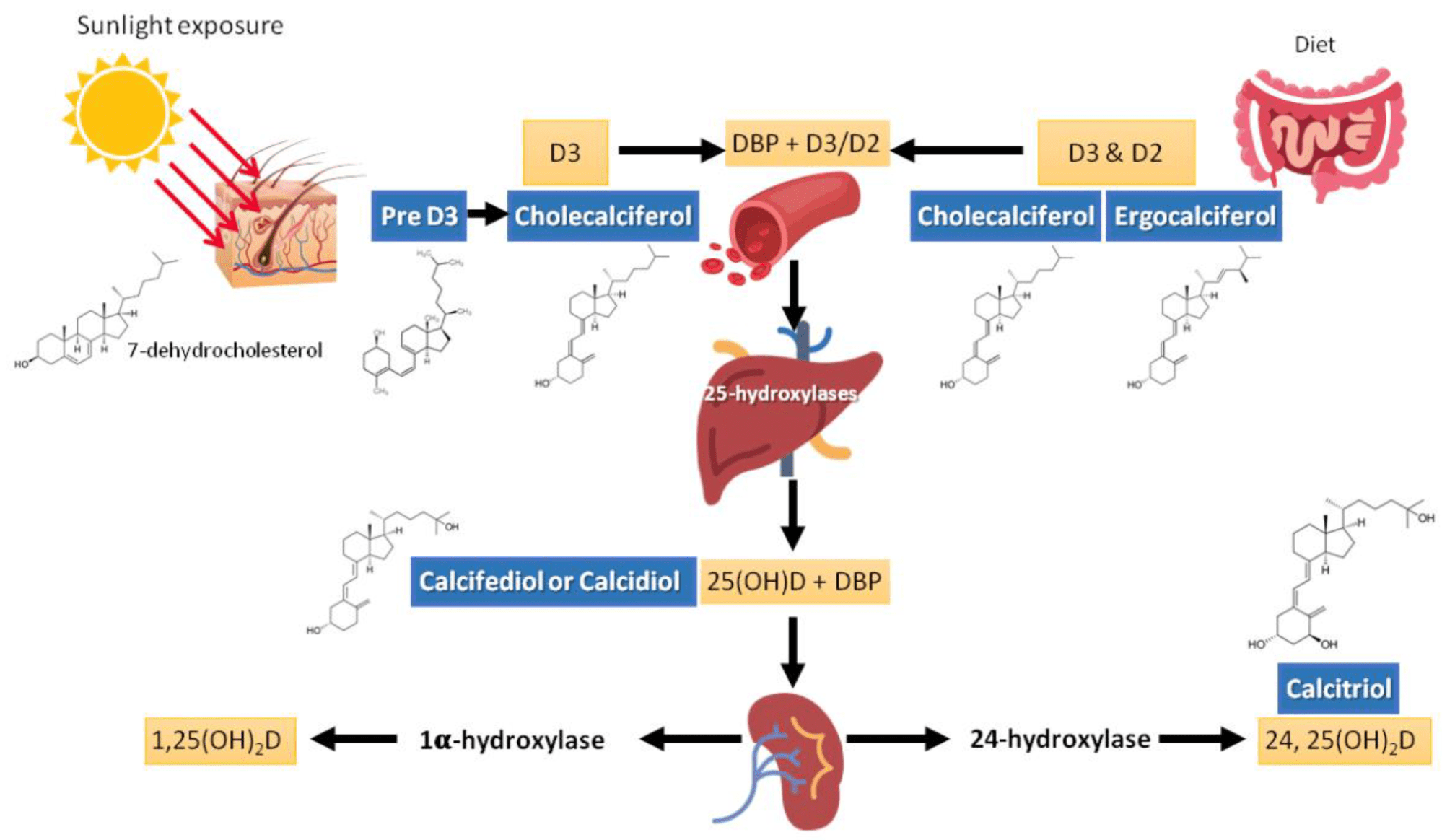
Both forms of vitamin D are biologically inactive when ingested and are absorbed in the small intestine. They are transported to the liver and converted into 25-hydroxyvitamin D (25(OH)D), also known as calcifediol or calcidiol, followed by conversion in the kidneys into 1,25-dihydroxyvitamin D (1, 25(OH)2D), or calcitriol, which is the biologically active form used by the body (Figure 1)3. Studies have shown that vitamin D3 leads to a greater increase of serum 25(OH)D than vitamin D25.
The ‘sunshine vitamin’ gets its name from the fact that it is also produced in human skin from 7-dehydrocholesterol when exposed to sunlight, or more specifically, UVB rays.
Functions
Research shows that vitamin D plays a significant role in bone health, muscle health and the immune system:
-
- Bone health: Vitamin D is a critical regulator of calcium absorption. In its active form, 1,25(OH)2D, it interacts with the vitamin D receptor (VDR) in the small intestine resulting in an increase in calcium and phosphate absorption2. However, calcium homeostasis is primarily regulated to maintain serum calcium within a narrow range for metabolic reasons with the parathyroid gland, bone, intestine and the kidney working together in this role4. Chronic vitamin D deficiency that results in an increase in parathyroid hormone leads to increased bone resorption, compromising the structure of the skeleton and increasing the risk of fracture thus vitamin D sufficiency is important to optimise skeletal health4.
- Immune health: Vitamin D plays a crucial role in regulating both the innate and adaptive immune responses. The expression of VDR in many different immune cells has been well demonstrated6. It modulates the activity of immune cells such as B cells, T cells and antigen-presenting cells and promotes a balanced immune response. Vitamin D deficiency is associated with an increased risk of hospitalisation for respiratory tract infections7 and supplementation has been shown to boost antigen-specific immunity in older adults with sub-optimal vitamin D status8. Genetic variation in the VDR genes has also been linked to Vitamin D deficiency and the development of autoimmune disease6.
- Muscle function: The identification of a VDR in skeletal muscle cells, along with the strong association between vitamin D deficiency, muscle atrophy and sarcopenia, suggests an important role in muscle function9. Proposed mechanisms include modulation of protein synthesis, mitochondrial metabolism and energy production, which may influence performance. However, the effects of vitamin D3 supplementation on muscle mass, strength and physical performance remain debated, with conflicting findings. Meta-analyses of randomised controlled trials in athletes have not shown conclusive benefits, highlighting the need for further research10,11. In contrast, supplementation has been associated with improved muscle strength in postmenopausal women12. Interpretation of trial results should consider whether populations have insufficient or sufficient vitamin D status and whether any supplementation used has increased 25(OH)D levels sufficiently as these factors may influence outcomes13.
- Mental health: Emerging evidence suggests a link between vitamin D and mental health – its neuroprotective properties may contribute to its role in mental wellbeing, reducing neuroinflammation, supporting serotonin synthesis and improving brain plasticity14. Recent meta-analysis suggests no benefit of supplementation in healthy individuals15 but potential effects on depressive symptoms in those with major depressive disorder or with milder, clinically significant depressive symptoms14. However, more high-quality research trials are needed.
- Other Potential Roles: Vitamin D has other roles in the body, including modulation of cell growth, neuromuscular function and glucose metabolism16. Ongoing research is also exploring the potential benefits on other health conditions including heart disease, diabetes and musculoskeletal diseases like multiple sclerosis17.
In European Union countries, approved health claims are available for the role of Vitamin D in supporting a wide range of functions including maintaining normal bones and teeth, muscle and immune function as well as supporting absorption of calcium and phosphorous subject to conditions.
In China, claims relating to the health of bones and teeth and the absorption and utilisation of calcium and phosphorus are also available for vitamin D containing foods subject to conditions.
Recommended Intakes
In some countries, national dietary reference tables can lag behind updated clinical practice or more recent Vitamin D supplementation policies.
-
- United States: The Institute of Medicine (IOM) Recommended Dietary Allowance (RDA) for vitamin D is 600 IU (15 micrograms) daily for adults aged 19–70 and 800 IU (20 micrograms) daily for adults over 70 years, assuming minimal sun exposure18.
- Europe: The European Food Safety Authority (EFSA) has set an adequate intake at 15 micrograms per day for healthy individuals over one year of age including pregnant and lactating women to ensure the majority of the population will achieve a serum 25(OH)D concentration near or above the target of 50 nmol/L19.
- China: The Chinese Nutrition Society have set a daily Reference Nutrient intake of 400 IU (10 micrograms) for adults aged 18-50 and 600 IU (20 micrograms) for adults over 50 years20.
Dietary Sources
Foods rich in vitamin D include oily fish (e.g., salmon, mackerel and sardines), egg yolks and offal. However, sources are limited and there are high levels of inadequacy of vitamin D intake globally21.
In some countries, fortification of staple food (e.g., milk, margarine, cereals) is used to increase vitamin D intake but these policies differ by region and are often voluntary, leading to variable dietary contributions. For this reason, local food composition data and values should be used when estimating intakes. For example, milk is frequently quoted as a source of vitamin D but only when vitamin D fortified milk is available. Liver is a source of vitamin D but is not widely consumed and is not recommended during pregnancy because of its high vitamin A content22. Among plant-based options, mushrooms exposed to sunlight or UV radiation can supply vitamin D2.
Vitamin D – Beyond Food
The level of 25(OH)D in populations varies geographically due to latitude, skin pigmentation, sun exposure, diet and supplement use. While endogenous production of vitamin D from sun exposure is also a potential source, recommendations to limit sun exposure to prevent skin cancer and limited sunlight in higher latitudes during winter mean that it cannot be relied upon as a source.

In many countries, vitamin D supplementation is recommended either during winter or throughout the year for more vulnerable populations (e.g. pregnant women, elderly, those with darker skin)23-25. The Endocrine Society also recommend supplementation for children aged 1 to 18 years and those aged 75 years and older as well as pregnant women and those with high-risk prediabetes26.
Vitamin D Deficiency
The concentration of 25(OH)D in blood serum is currently the main indicator of vitamin D status as it reflects vitamin D produced through both sunlight and from the diet. There is no universal agreement on the threshold for vitamin D ‘deficiency’. However, there is widespread acknowledgement of vitamin D deficiency using the most conservative 25(OH)D threshold of < 25/30 nmol/L, in both low- and high-income countries1. Depending on the world region, the prevalence of serum 25(OH)D below this threshold ranges from ~5 to 18% and 24 to 49% for levels below 50 nmol/L21.
Vitamin D deficiency in toddlers and young adults can cause rickets and slow brain development. Deficiency in adults causes osteomalacia (brittle bones) increasing susceptibility to fractures. Confirmed vitamin D deficiency is typically treated with high-dose supplements for a limited number of weeks followed by a maintenance dose28.
Excess Intakes
It is important to remember that as a fat-soluble vitamin, vitamin D can be stored in the liver and excessive amounts should be avoided. An upper daily limit of 100 micrograms from all sources has been set in the US by the IOM for those 9+ years18 while an upper daily limit of 50 micrograms for children and 100 micrograms for adults has been recommended by the EFSA27.
In Closing
Ongoing research continues to explore vitamin D’s potential benefits further refining our understanding of its role in human health. While vitamin D is essential, further research is needed to fully understand its role in various health conditions and to establish clear guidelines for supplementation.
This article was originally published on March 18, 2025 and updated on March 3, 2026.[/vc_column_text][/vc_column][/vc_row]
Nutrition is inherently multidisciplinary, drawing from the physical sciences, medicine, public health, psychology, sociology and increasingly, planetary health1. Therefore, nutrition science research is essential for advancing our understanding of human health and supporting evidence based decision making. Research in this space aims to clarify how nutrients, bioactives and other food components influence health, inform dietary guidance and policy and support strategies to prevent disease.
A wide range of study designs are used in nutrition research and no single study design can answer every question2. Understanding the purpose, strengths and limitations of each approach helps distinguish between stronger and weaker evidence, so the hierarchy of research methods is key to evaluating the quality of evidence.
This article outlines the key study designs used in nutrition research, the types of questions they are best suited to answer and the strengths and limitations that guide how their findings should be interpreted, based on several resources1-5.
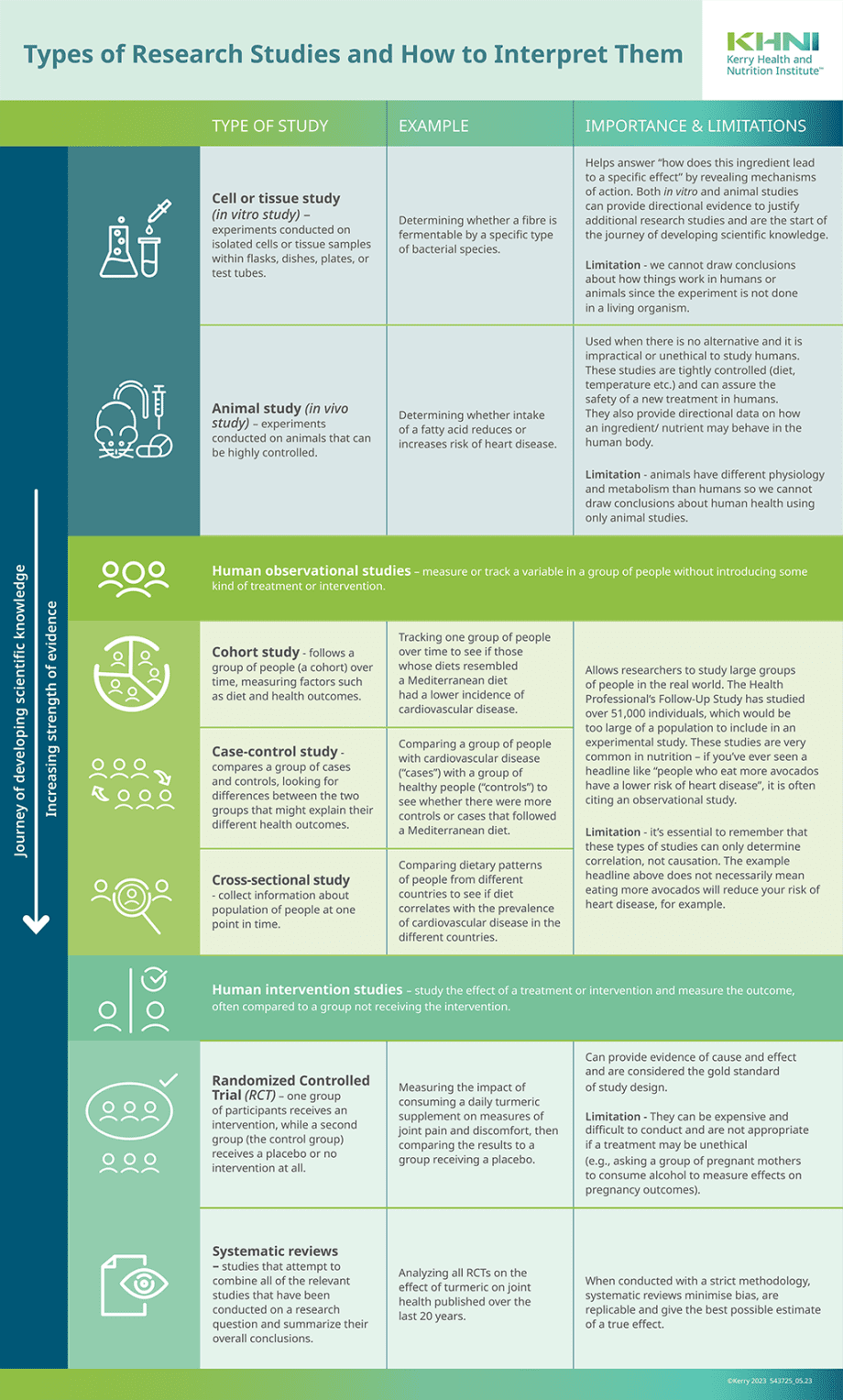
Visualising study designs as a pyramid (Figure 1) highlights how evidence strength varies. Studies at the lower levels of the pyramid tend to offer limited, less practical insights, while those at the top delivering stronger evidence with greater relevance to real world nutrition choices3,4.
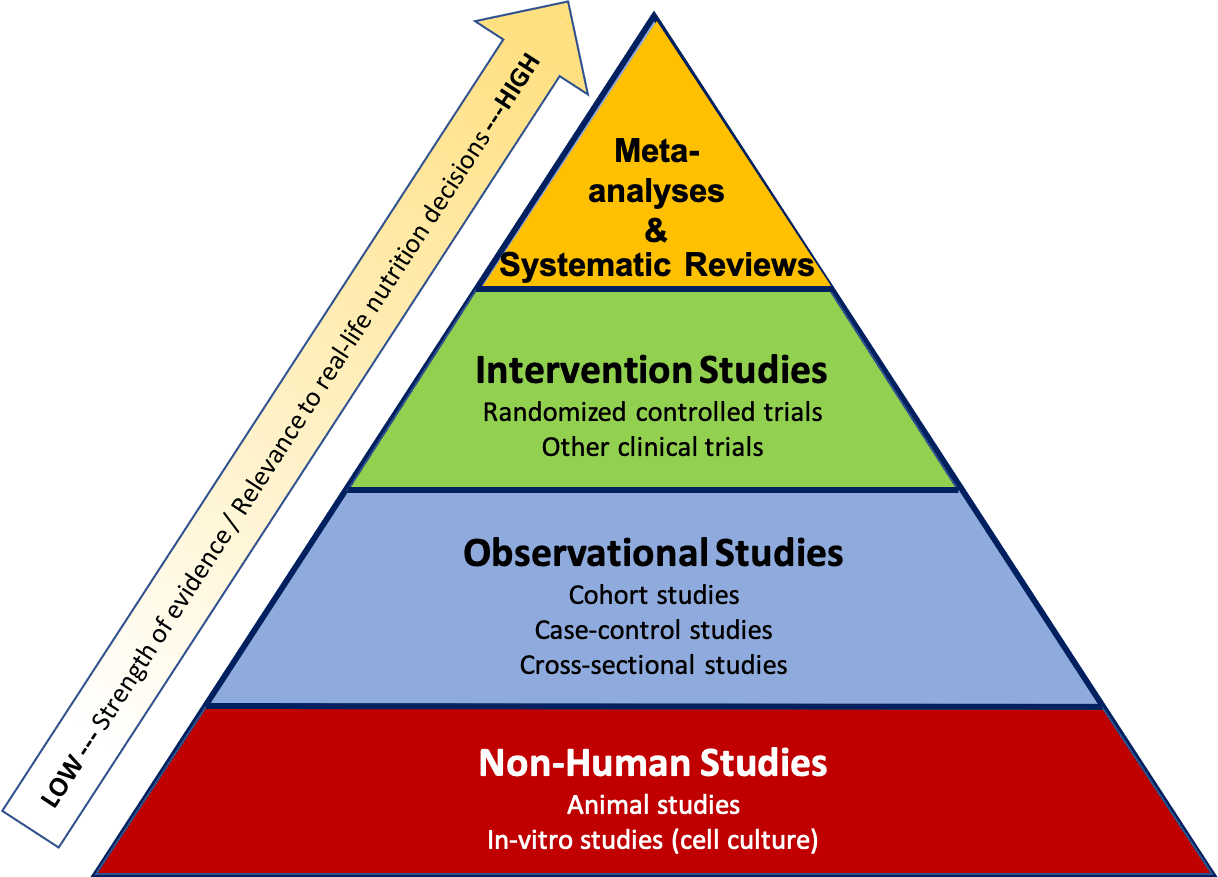
Figure 1. The hierarchy of evidence ranks different types of research according to the strength of the conclusions 3. (Licensed under CC BY 4.0)
Systematic reviews and meta analyses sit at the top of this hierarchy because they provide data across multiple studies to provide more comprehensive conclusions. Randomised controlled trials and prospective cohort studies typically provide the most robust evidence when examining relationships between dietary exposures and health outcomes. However, the rapid growth of the field — and the diversity of methods used — can make it challenging for practitioners and consumers to interpret findings and translate them into practice.
Foundational Research: Non-Human Studies
Foundational research — including in vitro studies in cells or tissues and in vivo studies in animal models — plays a critical role in uncovering the biological mechanisms that underpin how nutrients, ingredients and other food components behave in controlled settings. These early stage studies provide directional evidence that helps shape hypotheses and supports the rationale for human research.

It is important to note that isolated cells and tissues and animals do not replicate the complexity of human physiology. Differences in metabolism, exposure levels and biological responses mean that findings cannot be directly translated to human outcomes. For instance, a compound that influences cellular metabolism in vitro, for example, may behave very differently within the interconnected systems of the human body.
However, the value of foundational research becomes clear when it is integrated with human data. For example, while observational research links smoking with cancer, cell studies identify the carcinogenic compounds responsible. So, when mechanistic evidence aligns with human outcomes, confidence in the overall conclusion(s) is strengthened.
Observational Studies
These studies track large groups of people over time, in real-world settings, to understand how lifestyle behaviours — including dietary patterns — relate to health outcomes. These studies identify population level patterns and provide potential associations that warrant further investigation in more controlled study designs. Observational studies cannot determine cause and effect relationships and, hence, the impact of a single dietary or lifestyle factor.
Common observational designs include prospective cohort studies, case–control studies and cross sectional studies, each offering different strengths for understanding how diet and lifestyle influence long term health.
Case Control Studies
Case control studies compare people who already have a specific health condition (the cases) with similar individuals who do not (the controls). Researchers then look back in time to assess whether past exposures — such as dietary habits — differ between the two groups. For example, comparing fruit and vegetable intake in people with and without heart disease may help identify potential associations with disease risk.
These studies are relatively quick and cost effective, making them especially useful for investigating rare conditions or outcomes that would be difficult to study prospectively. They can also examine multiple potential risk factors at once and often serve as an important first step in identifying associations that warrant further research.
However, case control studies face several methodological challenges. Because exposure information is collected retrospectively, they are highly susceptible to recall bias — particularly when individuals with a disease remember past behaviours differently from those without it. Selection bias, confounding and reverse causation can also limit the strength of conclusions. For instance, if higher consumption of non sugar sweeteners is observed among people with obesity, it may reflect dietary changes made after weight gain rather than a causal effect of sweeteners.
Cohort Studies
Cohort studies are observational studies that are either prospective or retrospective, depending on when the data were collected. In a prospective cohort, participants complete questionnaires and undergo measurements at the start of the study. On the other hand, with retrospective cohort studies, researchers “look back” to analyse the relationship.
Prospective cohort studies follow large groups of people in real world conditions over many years — sometimes decades — to explore how dietary and lifestyle exposures relate to the development of diseases. Participants provide information at baseline and at regular intervals on factors such as diet, physical activity and health status. Dietary intake is usually self reported, which introduces challenges such as misreporting, difficulty estimating portion sizes and changes in behaviour over time.
By tracking outcomes over time, researchers can examine patterns and test hypotheses. Collectively, prospective cohort studies have shaped much of our understanding of how diet and lifestyle influence chronic disease risk, such as cardiovascular disease or osteoporosis. However, their long duration means they are time and resource intensive. As with all observational research, these studies can identify associations but cannot establish cause and effect relationships.
Cross Sectional Studies
This type of research provides a snapshot of health behaviours, exposures and outcomes in a population at a single point in time. They are typically conducted through surveys or brief assessments that collect information on both potential risk factors and health indicators simultaneously.
However, cross sectional research has important limitations. Because exposure and outcome are measured at the same moment, it is not possible to determine which came first. This raises the issue of reverse causality — for example, whether a dietary behaviour contributes to a health outcome or whether the health outcome influences how participants report their diet.
Cross sectional studies can also be affected by selection bias and recall bias, particularly when participants’ awareness of their health status shapes how they report past behaviours.
Despite these constraints, cross sectional studies are cost effective, relatively quick to conduct and useful for estimating the prevalence of dietary habits, lifestyle behaviours, or health conditions in a population. They can also highlight potential associations worth exploring in more rigorous study designs.
A typical cross sectional study might compare dietary patterns across countries to explore whether differences in diet align with variations in cardiovascular disease prevalence.
Randomised Controlled Trials (RCTs)
Randomised controlled trials (RCTs) are considered the gold standard for determining cause and effect relationships1,2,5.
Participants are recruited and randomly assigned to a control (placebo) group or an intervention group, ensuring the groups are comparable at baseline. For example, in an RCT examining the Mediterranean diet and cardiovascular risk, the control group might follow a standard low fat diet while the intervention group adopts a Mediterranean pattern3. After a defined study period, researchers compare outcomes such as heart attacks or strokes between groups.
Because randomisation minimises confounding factors, differences in outcomes can be attributed to the intervention itself. This is why RCTs provide the strongest evidence for causation rather than correlation. When conducted as double blind trials, neither participants nor researchers know who receives the treatment, further reducing bias and mitigating placebo effects.
Despite their strengths, RCTs come with practical and ethical constraints. They are expensive, often involve small sample sizes and may struggle with long term adherence, especially when testing complex dietary patterns. Ethical considerations limit the ability to test harmful exposures or withhold beneficial treatments.
Systematic Reviews and Meta Analyses
Systematic reviews and meta analyses sit at the top of the evidence hierarchy because they provide a comprehensive overview of existing evidence and can reveal whether findings are consistent across different populations and settings. However, these methods are only as strong as the quality and consistency of the studies they include and ensuring relevant studies are not missed or intentionally excluded.
However, these methods are only as robust as the quality and consistency of the studies they include and they rely on thorough, unbiased inclusion of all relevant evidence.
A systematic review uses a structured, transparent process to identify, evaluate and summarise all relevant research on a specific question. When the included studies are sufficiently similar in design, population and outcomes, researchers may conduct a meta analysis, which statistically pools results to generate a single, weighted estimate of effect. Larger, well designed studies contribute more heavily to this estimate than smaller or lower quality studies.
Systematic reviews and meta analyses help determine whether scientific findings are consistent, generalisable and reliable and they often guide policy decisions, clinical recommendations and future research priorities.
In Summary
Science is a continuous process. It can move slowly and often involves uncertainty, yet it remains the most reliable way to build understanding about the world and human health. Many types of studies contribute to this evidence base, each with its own strengths and limitations and no single study provides a definitive answer. Progress happens because researchers continually evaluate and refine one another’s work, identifying opportunities to improve methods and explore new questions.
The KHNI Health and Nutrition Megatrends, now in its eighth edition, highlights the scientific, technological, and consumer-driven changes redefining global food systems.
The quality of our sleep the night before a busy day can determine whether we are energized for success or end up feeling fatigued and unproductive. Having a sufficient and consistent sleep schedule is very important for our overall health and well-being. Sleep supports our brain function, our the circulatory system, our metabolism and our long-term memory retention1. Lack of sufficient sleep over time can lead to long-term complications, such as increased blood pressure and a weakened immune system2.
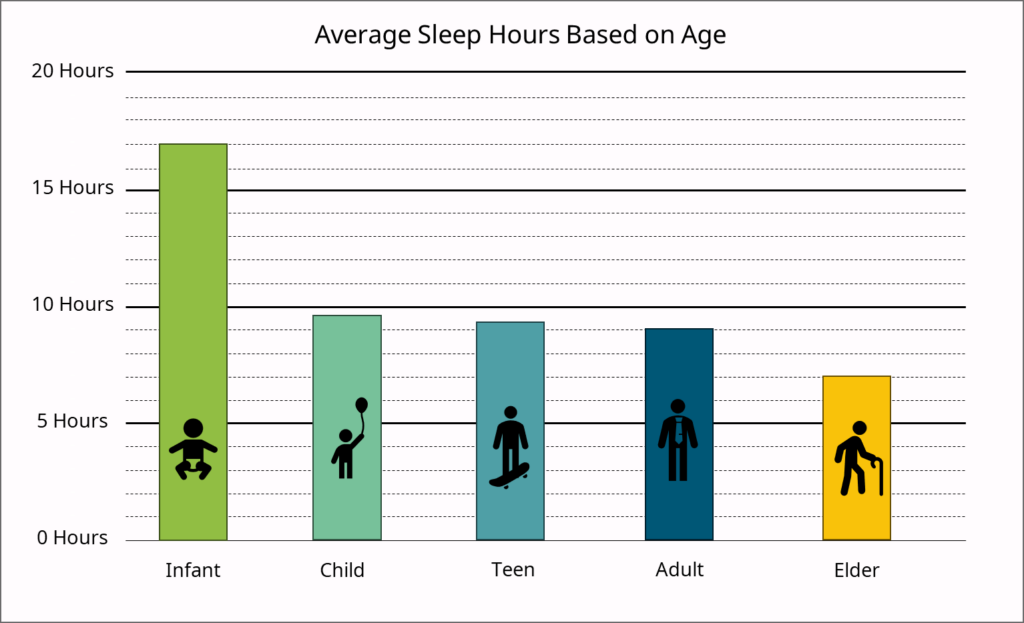
What does a Good Night’s Sleep Consist of?
The amount of sleep needed will depend on the stage of life and other factors such as activity level and certain co-morbidities. Babies initially sleep as much as 16 to 18 hours per day, which may boost growth and development (especially of the brain). School-age children and teens on average need about 9.5 hours of sleep per night. Most adults need 7-9 hours of sleep a night, but after age 60, night time sleep tends to be shorter.
Phases of Sleep
During sleep, our brains progress from two different sleep states: REM (rapid-eye movement) sleep and non-REM sleep.
-
- REM sleep occurs in the first 90 minutes after falling asleep. The body’s systems are more active compared to deeper states of sleep. This state almost mimics wakefulness as breathing is fast and irregular, heart rate and blood pressure are near waking levels. During REM sleep emotional experiences are processed and memories are consolidated. In addition to memory consolidation and emotional regulation, REM sleep also supports other cognitive functions such as mood stability, restorative brain activity, and brain development, especially in infants and children where neural pathways are growing and refining. Interestingly, REM sleep increases in duration in the latter half of the night, which is why we often wake up from a dream in the morning hours.
- Non-REM sleep follows as the brain gently drifts from a state of alertness to sleep, body temperature decreases and eye movements slow down. Brain activity occurs in small bursts and heartbeat and muscles relax further. The final stage of non-REM sleep is the deep sleep period. All systems slow even further, including brain waves. It can be difficult to rouse a person awake during this intense deep state of sleep3. Non-REM sleep contributes to physical repair and recovery, growth & development, supports immunity, regulates hormones and enhances memory consolidation.
Nutritional Interventions for Sleep Quality
Diet can significantly influence circadian rhythms and sleep quality. Nutrients that support the production of key sleep-related hormones, such as melatonin and serotonin, are particularly beneficial. Foods rich in tryptophan, an amino acid precursor to serotonin and melatonin, include turkey, chicken, nuts (especially almonds and walnuts), and seeds. These foods help regulate sleep-wake cycles by enhancing melatonin synthesis, which aligns with the body’s natural sleep rhythm.
Complex carbohydrates found in whole grains, oats, and legumes can improve tryptophan’s availability to the brain, promoting a restful sleep. Magnesium and potassium, present in foods like leafy greens, bananas, and sweet potatoes, also play a role in relaxing muscles and calming the nervous system, which is essential for preparing the body for sleep. Omega-3 fatty acids, found in fatty fish, like salmon and sardines, have been shown to support circadian alignment by influencing serotonin levels, which can improve sleep quality.
Vitamin B6 (in foods like bananas, chickpeas, and fortified cereals) and vitamin D (in eggs, fish, and fortified products) are essential for the synthesis of serotonin, helping to regulate mood and improve sleep quality. Additionally, antioxidant-rich fruits like cherries and berries contain natural melatonin, which may aid in promoting earlier sleep onset. Caffeine-free herbal teas such as chamomile and valerian root also have calming effects that can help with falling asleep and maintaining restful sleep.
Botanical extracts have been increasingly studied for their potential to support sleep quality. One such extract is Withania somnifera, commonly known as ashwagandha. Ashwagandha is considered an adaptogen, helping the body adapt to stress and balance the body’s physiological processes. While more research is needed, early studies have shown that ashwagandha may improve sleep onset, duration, and quality, especially in those experiencing stress-related sleep issues.
Both Alcohol and caffeine can significantly disrupt sleep quality. Caffeine stimulates the nervous system and acts as an adenosine receptor antagonist, blocking adenosine which promotes sleep. This causes an increase in alertness and delaying the onset of sleep. Consuming caffeine, especially in the afternoon or evening, can reduce the total sleep time and impair normal sleep14. Alcohol, while initially sedating, can lead to fragmented sleep and a reduction in REM sleep. It also disrupts the body’s natural temperature regulation and increases night time awakenings. Limiting both of these can help achieve more restorative and uninterrupted sleep15.

Sleep and Disease Risk
Insufficient or poor-quality sleep is increasingly recognised as risk factors for a range of chronic diseases. Studies have linked chronic sleep deprivation to elevated risks of cardiovascular disease, type 2 diabetes, obesity, and some neurodegenerative conditions. Disrupted sleep also impairs metabolic function, especially glucose metabolism and insulin sensitivity. Inadequate sleep has also been associated with increases in system inflammation and elevated blood pressure, both of which can contribute to cardiovascular risk. Poor sleep may also impact immune function, which increases the risk of infectious disease. Finally, lack of adequate sleep also contributes to increase in mental health risk such as stress, anxiety, and depression.
Emerging research continues to explore the significant role that diet plays in sleep quality. As we advance in understanding these connections, there is a growing opportunity for industries to implement evidence-based nutritional guidance and develop innovations, such as tailored meal plans and/or supplements, that support better sleep and overall health.
To help young athletes meet their nutritional needs and improve their performance, the Kerry Health and Nutrition Institute (KHNI), in collaboration with Kerry GAA, has launched a 3-part educational series titled ‘Food Fit for a Kingdom’. This series, hosted by John O’Connor, Head of Nutrition for Kerry GAA, and Aoife Marie Murphy, Senior Sustainable Nutrition Manager at the KHNI, offers practical advice on how to create balanced meals that fuel the high energy demands of youth athletes, regardless of their sport.
In the second video of the series, ‘Demystifying Nutrition’, John and Aoife visit young athletes at Kilmoyley and Cillard GAA clubs in County Kerry, Ireland, demystifying some nutritional myths and providing recipes to support their training and performance.
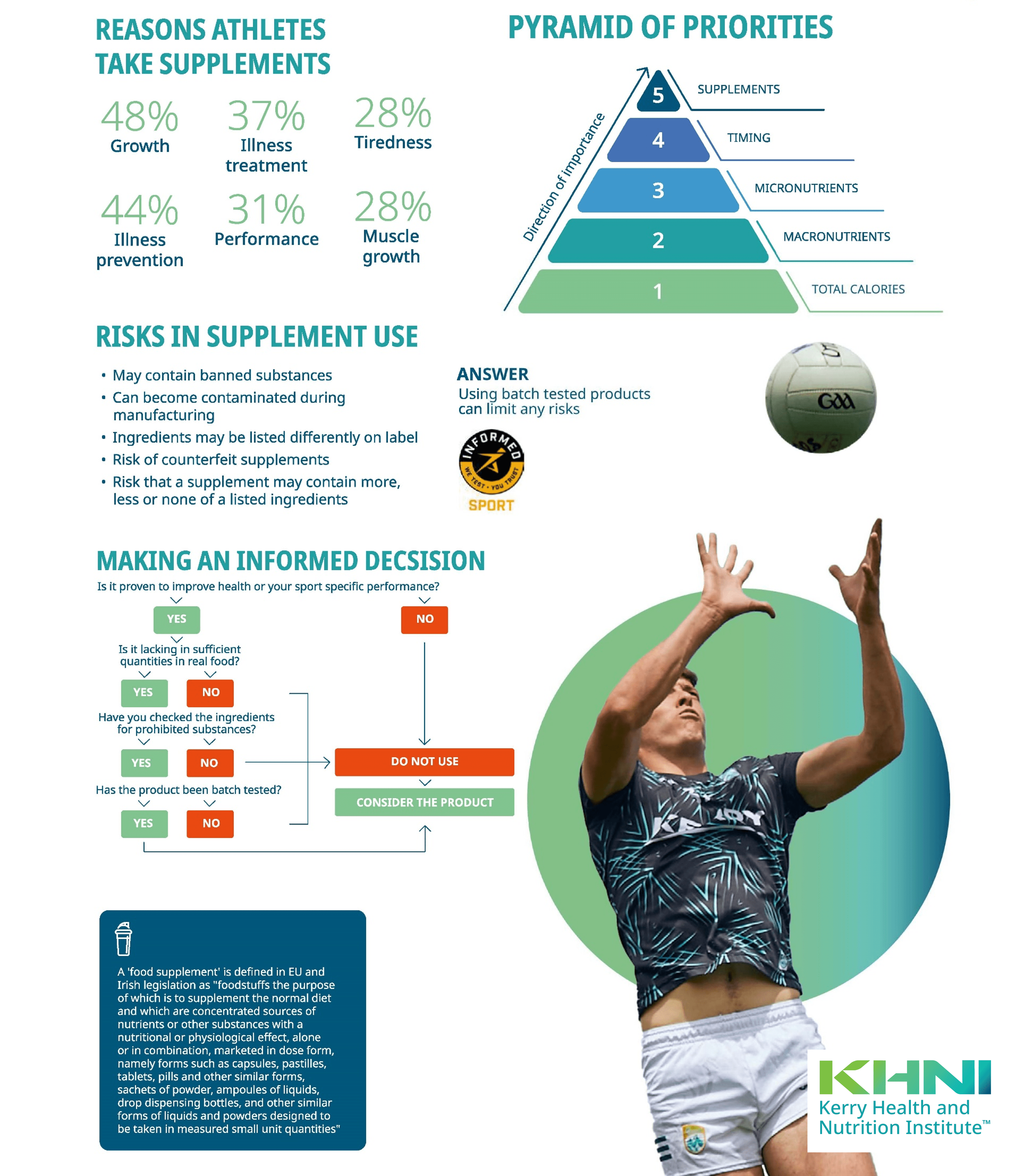
The Pyramid of Nutrition Priorities for Young Athletes
Proper nutrition is key to helping young athletes become stronger, recover faster, minimise injury, and maintain good health. It also boosts confidence and performance. The pyramid of nutritional priorities for young athletes is structured to highlight the most important factors for growth and success:
-
- Total Calories: The foundation of the pyramid, ensuring athletes get enough energy to support their high energy demands from physical activity and overall growth.
- Macronutrients: A balance of carbohydrates, proteins, and fats is critical for fuelling performance, muscle repair, and maintaining overall health.
- Micronutrients: Vitamins and minerals play a key role in energy production, immune function, and bone health. Eating a variety of foods rich in vitamins and minerals (particularly calcium, iron and vitamin D) will helps prevent deficiencies and supports overall health.
- Meal Timing: Eating at the right times—especially before and after training and matches—helps maximise energy levels and supports recovery.
- Supplements: Supplements should only be used when necessary, complementing a well-rounded diet, not replacing it. Certain nutrients like omega-3s and vitamin D may require supplementation, as they are harder to obtain from food alone. However, sports supplements are heavily marketed and should be used cautiously by young athletes.
For more detail on the nutritional requirements of young athletes see article Fuelling Fitness for Young Athletes – Kerry Health And Nutrition Institute
Understanding Sports Supplements
A “food supplement” is defined by EU legislation as any product designed to supplement the normal diet, providing concentrated nutrients or other substances that offer physiological effects. These products come in various forms, including capsules, tablets, and powders, and should only be consumed in small, measured quantities.
For growing teenagers, the use of sports supplements poses risks. Over-reliance on supplements can lead to an imbalanced diet, where nutrient-dense foods are overlooked. Furthermore, many supplements contain ingredients not fully tested for safety in younger populations, potentially causing adverse effects such as hormonal imbalances, liver damage, or dehydration. Some products may even contain banned substances, which can jeopardise an athlete’s eligibility in competitive sports. Therefore, it’s crucial for teenagers to focus on a balanced diet and seek guidance from healthcare professionals before considering supplements.

Making Informed Decisions About Supplements
When considering supplements, it’s important to make informed choices. If any of the following questions cannot be answered with a confident “yes,” it’s advisable to avoid using the product:
-
- Is the supplement or active ingredient clinically proven to support health or performance?
- Is the ingredient lacking in sufficient quantities in whole foods?
- Has the supplement been checked for prohibited substances?
- Has the product been batch-tested?
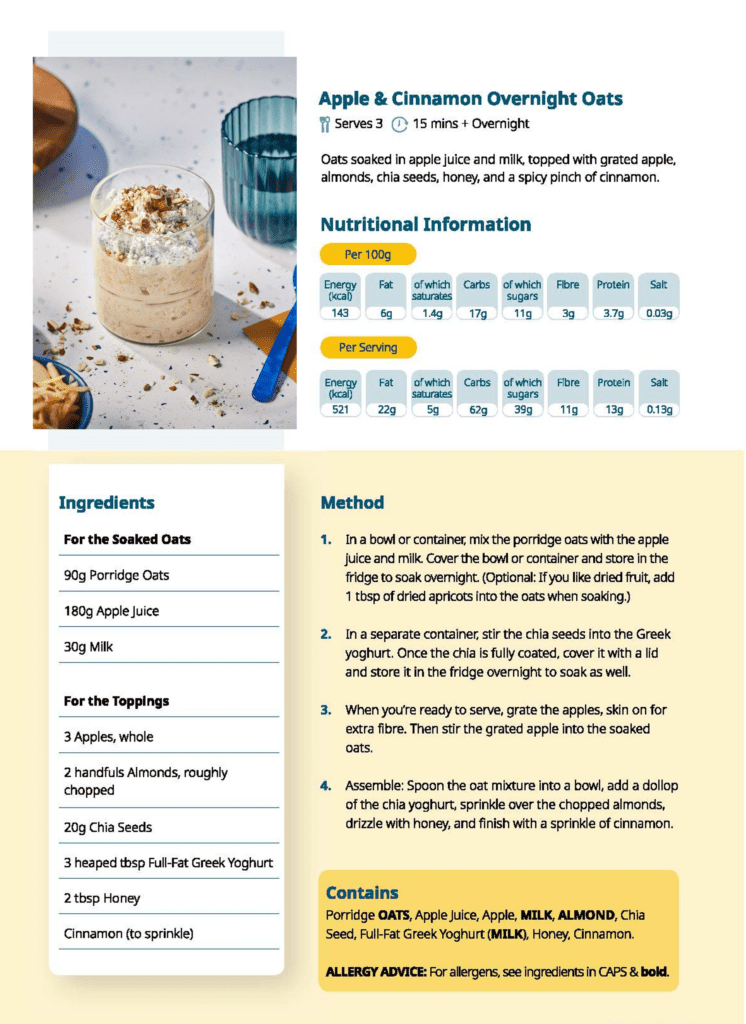
See recipes idea’s for young athletes to obtain the nutrients they need for training.
Conclusion
With the abundance of nutritional advice available, it can be overwhelming for young athletes to navigate their choices. The pyramid of nutritional priorities offers a helpful framework to prioritize the most important aspects of nutrition for peak performance and recovery. While marketing and influencers may place undue emphasis on the need for supplements, a food-first approach is always the best strategy. When supplements are necessary, it’s vital to choose high-quality, well-tested products.

Vitamin B12 is a water-soluble vitamin, also known as cobalamin, this cannot be made in the body and needs to be ingested through food, supplements, or medication. It is essential for red blood cell formulation, keeping your nerve and brain function healthy, production of DNA, and maintaining cell metabolism.
Vitamin B12 is absorbed by the stomach with the help of a protein named intrinsic factor which is a glycoprotein, this protein substance binds to the B12 molecule and aids in the red blood cells absorbing it. Excess B12 can be stored in the liver for future use or excreted through urine.
With more consumers choosing plant based diets or veganism, meeting essential B12 requirements can sometimes be challenging. Unlike many essential vitamins that can be readily sourced from plants, Vitamin B12 is primarily found in animal products, making it difficult for vegans and vegetarians to obtain adequate amounts of through their diet alone. Understanding the role of Vitamin B12 in the body is crucial for maintaining optimal health and wellness.
How much Vitamin B12 do we need and where do we find it?
The Recommended Daily Intake (RDI) of Vitamin B12 is 2.4 micrograms daily for adults and children over the age of 4 years old. Those who are vegetarians, vegans, pregnant and breastfeeding may need to increase their intake slightly or could run the risk of deficiency. Older adults, those with intestinal issues, those who are Pregnant and Breastfeeding, Infants of Vegan and Vegetarian mother’s, Vegetarians and Vegans are all at higher risk for developing a deficiency in B12. It was also reported that 1 in 10 adults over 75 years, and 1 in 20 adults aged between 65-74 years had a deficiency of Vitamin B12.
B12 can naturally be found in foods of animal origin such as meat, fish, eggs and dairy products, specific examples include animal liver and kidneys, beef, tuna, salmon, broccoli, peas, and brussels sprouts. It can also be added to fortified nutritional yeasts and fortified breakfast cereals. In cases of Vitamin B12 deficiency, it can also administered in the form of supplements and injections.

What happens if we do not have enough Vitamin B12 in our diets?
Insufficient intake of Vitamin B12 can lead to deficiency. This can occur when Vitamin B12 levels in the blood drop, resulting in metabolic abnormalities. These abnormalities lead to the onset of physical and psychological symptoms, such as as nausea, constipation, diarrhoea, metal health issues, low red and white blood cell count, deterioration in walking, vision impairment, and fatigue. The long-term symptoms of include, pernicious or macrocytic anemia, heart conditions, temporary infertility, and issues with the nervous system. If untreated, this can then result in the development of pernicious or macrocytic anemia.
Pernicious anemia is when the immune system attacks the healthy cells within the stomach which results in a lack of absorption of Vitamin B12 in the body. Macrocytic anemia is when the body produces abnormally large blood cells that lack the required nutrients and do not function as they should. Vitamin B12 deficiencies are treated by taking supplements or Vitamin B12 injections (hydroxocobalamin) depending on GP advice and the severity of your deficiency. Supplements/injections may be required long-term if symptoms persist. However, a beneficial start to improving Vitamin B12 levels in the body is to consume a high about of Vitamin B12 rich foods.
The preventative steps we can take to avoid a Vitamin B12 deficiency is to consume foods rich in B12, as listed above. Additionally, a deficiency in Vitamin B12 may not always be due to an inadequate dietary consumption of foods containing B12, it is possibly due to the lack of the intrinsic factor, this is most common among older adults which is associated with an autoimmune disease called pernicious anemia.
|
Get KHNI articles delivered to your inbox
|
How Does Vitamin B12 interact with other Vitamins?
It should be noted that taking Vitamin C in close proximity to Vitamin B12 foods/supplements should be taken with caution as Vitamin C can reduce the amount of B12 in the body, therefore spacing out the consumption of both vitamins is recommended.
Vitamin B12 and Folate (B9) work together to produce a compound that aids in immune functionality, and red blood cell formulation. Therefore, consuming a balanced amount of foods containing B12 and Folate is beneficial for the overall health. It should also be noted that consuming over 1mg of folic acid daily can mask the symptoms of a Vitamin B12 deficiency.

Vitamin B12 Production Process and Sustainability:
For those who can’t get enough Vitamin B12 through their diet, supplementing B12 may be necessary. Supplemental Vitamin B12 is produced commercially through a bacterial fermentation process, taking up to two weeks from beginning to final product. It is one of the most complex vitamins to produce beginning with bacteria growing in large vats holding over 100,000 liters, this amount still only produces a small yield of final product. It is not a sustainable process and can be harmful to the environment as it traditionally uses cobalt and cyanide, and the harmful and hazardous surplus is expensive to be disposed of to ensure environmental health measures are not affected.
Research from the University of Kent took place in 2023 to develop a sustainable manufacturing process for Vitamin B12. The team manufactured a strain of E-coli that contains a smaller amount of cobalt that is then absorbed during the production process and there is no surplus cobalt left to be disposed of, therefore it is not a high health or environmental risk and is less of an expense. This is a step in the right direction and is a template that other bacterial processes could benefit from and become more sustainable in the future.
Vitamin B12 plays a vital role in the functionality of a healthy body. Ensuring a holistic diet to include certain meats, dairy products, fish, and certain vegetables will help reduce the risks that come with its deficiency. Increasing the availability of knowledge surrounding the importance of Vitamin B12 and its sources would advocate for a better understanding among individuals. This in turn will reduce the risks associated with lower consumption of this vital vitamin. Additionally, looking towards the future of supplemental B12 production, a long-term plan to formulate a universal sustainable production process of Vitamin B12 would reduce the harmful environmental impact and costs all while benefitting those with a deficiency.
Do you know your pro-biotics, pre-biotics, botanicals and supplements, from your vitamins, macro-nutrients and micro-nutrients? All can help women manage their physical and emotional wellbeing, but what should you consider taking and when?
“Nutrition plays a role in women’s health, both in managing different life stages and in promoting long-term health, but with so many options available it can be overwhelming,” says Dr. Karin Dorrepaal, Independent Non-Executive Director at Kerry.
“At Kerry, we have a dedicated team of scientists and experts in women’s health, so we’ve called on them to bust some myths, navigate the science on what actually works, and tell us how nutrition can support health and quality of life throughout a woman’s life.”

Women’s unique nutritional needs
“When you consider the various stages of a woman’s life, adolescence, reproductive age, pregnancy, lactation, peri-menopause, menopause and post-menopause, it’s not surprising that each of these stages requires distinct nutrition to support overall wellbeing. For example, adolescent females have an increased requirement for calcium to build life-long bone density. A deficiency in calcium at this life stage can result in increased risk of osteoporosis post-menopause, when the protective effects of estrogen decline,” said Dr. Lisa Ryan, Head of Department of Sport, Exercise and Nutrition at Atlantic Technological University in Ireland, and Scientific Advisory Council member of Kerry’s Health & Nutrition Institute (KHNI).
By understanding the specific nutritional requirements of each life stage, women can make informed choices about their own health. This article focuses on fertility, pregnancy and breastfeeding, and menopause, and looks at how nutrition affects these life stages.
Nutrition and fertility
 One in six women experience infertility. Hormonal imbalances can disrupt a woman’s delicate reproductive process, leading to irregular cycles, failure to ovulate (anovulation), difficulty conceiving, or infertility.
One in six women experience infertility. Hormonal imbalances can disrupt a woman’s delicate reproductive process, leading to irregular cycles, failure to ovulate (anovulation), difficulty conceiving, or infertility.
There are some unknown causes of infertility, but one in three cases of female infertility is caused by polycystic ovary syndrome (PCOS) – the most common hormonal disbalance affecting women.
What is PCOS?
Polycystic ovary syndrome (PCOS) is a common condition that affects how a woman’s ovaries work. Polycystic ovaries are bigger than healthy ovaries and have twice the number of follicles than healthy ovaries do. In PCOS ovulation doesn’t take place each month causing women to stop having periods or have irregular periods and can also cause fertility issues. It’s a complex, chronic condition associated with a range of endocrine and metabolic symptoms. It can have a profound impact on a woman’s health, fertility, self-esteem, and body image, leading to emotional distress. PCOS is not just a fertility issue but one affecting a woman’s overall health, including her mental wellbeing. PCOS is leading cause of female infertility (PCOS is responsible of 25-40% of cases).
“The exact cause of PCOS is unknown. It’s thought to be linked to abnormal hormone levels in the body, including high levels of insulin. It is also related to a deficiency in inositol (a sugar made in the body and found in foods) and specifically a systemic deficiency in the D-chiro-inositol and ovarian deficiency in Myo-inositol. Women with PCOS need to ensure an adequate intake of inositol through their diet or consider taking a supplement,” said Dr. Monica Maria Olivares, RD&A Director for Women’s and Infant Health at Kerry.
Monica added: “The benefits of inositol in PCOS are very well known there are more than 300 scientific publications about this topic, more than 50 clinical trials, and 20 metanalysis demonstrating the benefits of inositol on fertility, skin, cardiovascular disease, hyperandrogenism and hyperinsulinemia.”

Nutrition in Pregnancy and Breastfeeding
“The first 1,000 days of a child’s life – beginning with conception through the first two years of childhood – critically impact development and health throughout life. Therefore, it is essential that women have the nutrition, care, and the support they need for the healthiest possible future for themselves and for their children,” said Dr. Izaskun Monsalve, Marketing Manager for Women’s Health at Kerry.
Vitamin and mineral needs can vary greatly between pre-pregnancy, pregnancy, and lactation. A carefully chosen diet can meet recommendations for most nutrients, but the diets of pregnant and lactating women often fall short of many essential nutrients. For example, many pregnant women under-consume:
-
-
- folic acid (to help protect against neural tube defects);
- choline (for fetal brain and nervous system development);
- iron (for increased maternal and fetal blood volume); and
- calcium (for bone growth and reduced risk of maternal hypertension).
- Omega-3 (for fetal brain and eye maturation)
-
During lactation, the mother is able to provide all of a child’s nutrient needs via breastfeeding. For optimal health of the infant, the World Health Organization (WHO) recommends exclusive breastfeeding for the first six months. For the mother, this means that the required intake of many nutrients becomes even greater than during pregnancy – after all, the baby is still totally dependent on the mother for nutrition, but it is now bigger than it has ever been. As a result, it is essential for the mother to eat a balanced diet during this time to ensure both she and her baby are healthy. For some nutrients, the mother’s body will ensure the breast milk contains enough for the baby even at the risk of depleting her own body’s reserves. These are mostly nutrients that are absolutely essential for proper growth and development of the baby, such as protein, calcium, and zinc. Inadequate intake by the mother could lead to higher risk of iron deficiency, anemia, or loss of bone mineral density.
Some mothers don’t get the support they need to  sustain breastfeeding. Mastitis is the leading medical cause of women ceasing breastfeeding with ~15% of women experiencing mastitis during breastfeeding. The main symptom is pain.
sustain breastfeeding. Mastitis is the leading medical cause of women ceasing breastfeeding with ~15% of women experiencing mastitis during breastfeeding. The main symptom is pain.
“Many women are told that pain is normal during breastfeeding. It’s not true,” according to Izaskun. “Pain is not normal in breastfeeding. Pain is often caused by mastitis, it is a problem, and in most cases it can be easily managed by treating the cause of the mastitis with a natural probiotic.”
She continued: “We were the pioneers in investigating probiotics in human breast milk and after extensive research our R&D team isolated the first strain from women’s breast milk and it has been shown to be effective in reducing mastitis and significantly reducing the pain symptoms of mastitis in three clinical trials, involving more than 1,000 women.”
What is mastitis?
Mastitis is an inflammation of breast tissue and is associated with an imbalance of the microbiota of the mammary gland. The main symptom is pain, and the pain, heat and swelling can be very intense. Other symptoms include inflammation and obstruction of mammary ducts, and it can be associated with systemic symptoms like fever and tiredness. Mastitis a very common problem during breastfeeding, affecting around 15% of women.

Nutrition in Menopause
Peri-menopause, pre-menopause, menopause, post-menopause. The menopause isn’t a single event in a woman’s life, but something women experience over the course of a couple of decades. It’s a transformative phase, marking the end of a woman’s reproductive years. This natural transition brings about a myriad of changes, both physical and emotional.
1 billion women worldwide will be experiencing menopause in 2025. 80% of them will have menopausal symptoms, symptoms that can severely impact their quality of life.
“I really believe that helping women achieve real understanding of how their hormonal health impacts their overall health can increase positive sentiment and have a hugely positive impact on women’s lives,” said Izaskun.
What is the menopause?
Menopause is the consequence of the reduction in the ovarian function as it’s a gradual decrease in the level of estrogens in a woman’s system. Estrogens regulate the growth development and physiology of the human reproductive system, but also are involved in neuroendocrine, skeletal, adipogenesis and cardiovascular system. The low level of estrogen during menopause reduces the activation of estrogen receptors and causes the symptoms associated with menopause.
There are more than 30 different symptoms associated with the menopause. Common symptoms include:
-
-
-
- hot flushes
- night sweats
- difficulty sleeping
- fatigue
- lack of energy
- low mood or anxiety
- problems with memory or concentration
- vaginal dryness and pain, itching or discomfort
- reduced sex drive (libido)
- discomfort during sex
- irregular periods
- headaches
- heart palpitations
- recurring UTIs
- loss of muscle
- weight gain, and
- joint aches and pains.
-
-
Women choose to manage their symptoms and look ahead to healthy ageing in many different ways – pharmaceutical treatments, herbal remedies, life-style changes and increasingly nutritional changes, like adding more phytoestrogens to their diet.
Monica said: “Phytoestrogens are plant-based compounds that mimic the effects of estrogen in the body. They occur in different botanicals, for example in red clover, soybeans and hops, and have been shown in clinical studies to reduce the frequency and intensity of menopause symptoms without serious side effects, which is very important. In fact, there are more than 1,500 scientific publications, 300 clinical trials, and 30 metanalysis demonstrating how phytoestrogens can help to address symptoms in menopause.”
Lisa added: “There are also specific nutritional considerations for post-menopausal women. For instance, many experience changes in taste perception and suffer from severe dry mouth. Their food preferences may shift, and they may require different supplements or novel botanicals to support these changes. This presents opportunities for food and nutrition innovation specifically tailored to women’s health.”
Conclusion
There is a growing recognition of the unique health needs of women and a shift toward prioritising women’s wellbeing. “This increased awareness and advocacy have created a demand for more comprehensive research and solutions. With women’s health spanning from adolescence to old age, innovative technologies, treatments and products are being developed to address various aspects of women’s health,” said Karin.
That said, every woman is different, and their needs are distinct and unique throughout various stages of life. Nutrition therefore needs to be personalised. Izaskun illustrates the point: “If we take menopause for an example, we’re talking about 30 different symptoms that affect women in greater or lesser extent. So, for each woman it’s a different experience. Women need specific solutions for the symptoms they are experiencing.”
New technology is making personalisation easier. By tracking what happening in their bodies, women can better understand the symptoms they are experiencing, allowing them to make decisions about taking a specific diet or ingredient to meet their individual needs.
“There is wealth of information available about how women can use nutrition to manage their physical and emotional wellbeing throughout their lives. What’s important is to seek out science-based information and products that have been tried and tested in clinical studies,” concluded Lisa.
For more scienced-based information about the nutritional needs of women subscribe to KHNI.
October 18th is World Menopause Day. It’s a day to come together an recognise the significance of menopause in the lives of women worldwide. With the importance of Women’s Health across the life stages, we would like to share key insights from our women’s health webinar that explored the intricate relationship between menopause, health, and nutrition.
Menopause is an inherent and transformative phase in a woman’s life. This natural transition brings about a myriad of changes, both physical and emotional. Our webinar delved into the diverse aspects of menopause, shedding light on its impact on women’s overall well-being.
In the video from the webinar, our experts Dr Izaskun Monsalve and Dr Monica Maria Olivares discuss the science behind menopause and the opportunities to innovate. More importantly, they explored the crucial roles that health and nutrition play in managing symptoms and promote long-term health.
Join us on this informative journey as we celebrate World Menopause Day by fostering awareness and encouraging informed choices.
Together, let’s embark on this journey towards better health and well-being for women globally.
Likely since the start of the current pandemic you have given some thought to your immune system and just how well it is functioning. If you’re like many others during those first months of the pandemic you turned to internet searches to learn more about your immune system and what proactive steps you could take to support its functions. During those searches, one of the terms that you may have encountered was “immunomodulators used with words like “nutrition” and “diet” or “food”. Why is this? And can food we eat really have immunomodulatory effects? In a word, yes.

What are immunomodulators?
An immunomodulatory compound, also called a biological response modifier or BRM in the pharmaceutical industry, is one that has the capacity to interact with the immune system in a specific way, altering the outcome of specific immune processes. The resulting changes could be either an increase or decrease in function depending on how much of the immunomodulator was consumed or administered as well as how that specific immunomodulator interacts with the immune system. Immunomodulatory compounds can be produced either endogenously (inside the body) or exogenously (outside of the body). Endogenous immunomodulators are compounds normally found within our body such as cytokines, hormones and growth factors. Exogenous immunomodulators can be synthetic (many prescription medications) or naturally occurring such as ingredients in our foods and nutritional supplements. Some of these ingredients are familiar, such as vitamins and minerals which are commonly understood to be necessary for the proper functioning of our bodies.1 For example, zinc helps activate and regulate immune cells so they can perform their job in the body.2
Examples of immunomodulators
 Omega-3 and omega-6 polyunsaturated fatty acids
Omega-3 and omega-6 polyunsaturated fatty acids- Carbohydrates such as glucans, mannans, fucoidans, fructans, xylans, and pectins
- Yeast beta-glucans
- Plant components such as astragalus root or echinacea flower, to varying degrees
There are many other types of naturally occurring compounds found in the foods and supplements we consume which have at least some scientific evidence that they have immunomodulatory activity. Many of these ingredients are plant-sourced and can be easily consumed in foods and nutritional supplements. Examples include omega-3 and omega-6 polyunsaturated fatty acids (PUFA) such as linoleic acid and oleic acid which are proposed to have anti-inflammatory effects in humans.3 The more familiar fatty acids, docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) have been studied for a wide range of biological effects, including immunomodulation but are sourced mainly from marine animals.4 Plant-derived polyphenols such as curcumin and quercetin have been tested in human clinical trials for immunomodulatory (generally anti-inflammatory) activity as well as other biological effects.5
Some of the most well-studied immunomodulatory food ingredients are polysaccharides, a type of carbohydrate. Polysaccharides that have been examined for immunomodulatory activity mainly fall into six types: glucans, mannans, fucoidans, fructans, xlyans and pectins and galactans.6 Some of these polysaccharide ingredients are well known such as pectins, glucans and inulin (a fructan) for being dietary fibers. Others, such as carrageenan (a galactan), have been used as emulsifiers and texturants in foods for decades. Many of these polysaccharides seem to have immunomodulatory properties that have been examined with various degrees of scientific rigor.7
How do immunomodulators work?
A case study with beta glucan
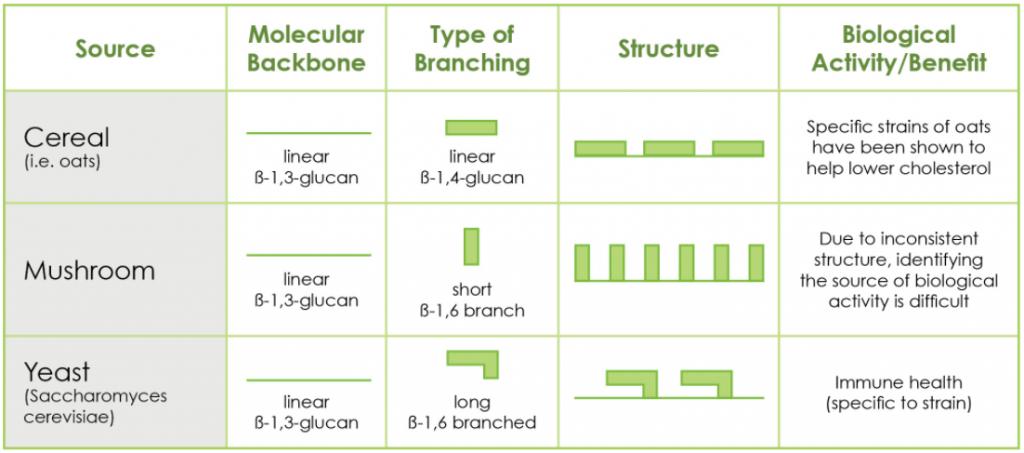
A polysaccharide of particular interest due to the observed positive effects on health, more than 75-year history of scientific study and overall robust scientific data portfolio is beta glucan. Beta glucan occurs naturally in many different types of organisms ranging from yeast to mushrooms to bacteria and plants such as algae and cereal grains.
The beta glucans produced by these different organisms vary in chemical structure depending on which organism made it, and science shows that the biological activity a beta glucan has in the human body is linked to its specific structure.8 Because of this structure-activity relationship inherent in beta glucan biology, it is essential to clearly identify the source and chemical structure of a beta glucan when seeking out an immunomodulator food ingredient since not all beta glucans have immunomodulatory properties.9
Breaking down the structure
Beta glucans are long chains of sugar molecules linked by one of three types of chemical bonds from which they derive their name (β-(beta)1,3; -1,6 or β-1,4). You will see beta glucans commonly described based on their chemical linkage patterns. Yeast beta glucan (called β-1,3/1,6 glucan) is one of the most well studied types of immunomodulatory beta glucans. It has a linear β-1,3-linked backbone with long β-1,3-linked branches connected through β-1,6 linkages. It was identified as the primary immunomodulatory component of yeast in laboratory experiments approximately 80 years ago 10 and has been characterized in increasing detail through subsequent decades. Once scientists discovered the receptors that recognize yeast beta glucan in our body and allow it to bring about its effects on health, called CR311 and Dectin-112, great progress has been made toward a detailed understanding of how yeast beta glucan exerts its immunomodulatory effects.
Innate immune training and yeast beta glucan
Experts in the field currently understand that yeast beta glucan modulates the immune system partially through a phenomenon referred to as innate immune training.13 Innate immune training is the term used to describe the priming of the innate immune system by some types of immunomodulators. This concept can be understood by comparing it with the more familiar concept of immune memory. Immune memory occurs when we are infected with or vaccinated against a pathogenic organism (eg measles or whooping cough). Our immune system recognizes the challenge and fights it off, making antibodies in the process. The cells that make these specific antibodies stay in the body long-term and will respond quickly to that same pathogen if it were to enter the body again, which typically prevents further symptomatic infections from that pathogen.

In contrast, the innate immune system works on a shorter time frame but can still be trained by that same encounter with the pathogen described above. Instead of “remembering” that specific pathogen for a lifetime, innate immune cells become primed for an extended period of time (months to a year), or ready to respond to the next threat (of any type) more effectively than when the cells were not primed. In this case, the pathogen would have modulated the immune system to be more effective at fighting off a specific pathogen. This training effect has been shown to have real impact on human health, for example reducing all-cause mortality in the first two years of life for infants vaccinated with the tuberculosis vaccine.14 Encouragingly, in the last decade it has been recognized that the innate immune system can also be trained by encountering compounds that are not from pathogenic organisms such as beta glucan from baker’s yeast.15,16 This means we could experience a similar training effect from consuming food instead of being infected by a pathogen.
Innate immune training could be compared to a recreational athlete training for a more intense event such as a marathon. Imagine you are the athlete. You don’t know specifically what kind of weather and race conditions you will encounter on the day of the race but you have a set of skills that will get you through the race (running pace, mental strength, breathing techniques, etc.). You can prepare yourself to use these skills most effectively on the day of the race by training generally to run the distance in varied weather or terrain conditions. The goal of the regular training is to ready (prime) all your skills to perform at your best and complete the race to the best of your ability no matter what race conditions you encounter (challenge).
Ways yeast beta glucans can act as immunomodulators
Immune training by certain yeast beta glucans works in a similar way. The immune system cannot predict what the next challenge encountered will be, but when the innate immune system is trained by yeast beta glucan, innate immune cells are primed to activate the defense skills they possess (similar to run pacing, mental strength and breathing techniques for the athlete) more efficiently in order to combat the threat. Think of primed cells as ready for action but not yet acting in the absence of a threat.
There are a plethora of scientific studies describing the effects of yeast beta glucan on the immune system. A few highlights include studies reporting
-
- increased potential for producing the innate immune system’s chemical weapons (reactive oxygen species)17
- increased capacity to produce cytokines important for an effective immune response15,18
- increased speed and directionality of innate cells migrating toward a pathogenic challenge19-21
- enhanced engulfment ability (phagocytosis) of foreign challenges22
- reversal of experimentally-induced immune suppression23
- enhancing the body’s ability to make more innate immune cells.24
This increased readiness of multiple immune defense functions likely results in the effects observed in numerous clinical trials, showing improved outcomes in upper respiratory tract infections, an indicator of immune system efficacy. 25
Constant research is being done to understand the mechanisms of action of immunomodulators, so expect to see more studies in the future describing how these components of food can support immune health.
How can the foods we eat influence our mood? Has science been able to explain a link between food and mood?
In this KHNI Q Science Short, Aoife Marie Murphy, PhD answers these questions and more. Watch the video to learn about:
-
- How food and nutrition can support different mood states like energy and relaxation
- Areas of emerging science on food and mood, like the gut-brain axis and nootropics
- Three simple dietary changes that science shows can improve mood
KHNI Q is a video series where scientific experts demystify the science behind healthier food.
Addressing sustainable nutrition is central to the future of the food and beverage industry. Many companies are transforming their strategies to improve measures such as water use, carbon emissions, animal welfare, and food waste while also addressing societal challenges such as obesity and malnutrition.
However, addressing sustainable nutrition can often come with unique taste and mouthfeel challenges. The phrase “the least nutritious food is the one that goes uneaten” emphasises the importance of understanding taste science as a tool to achieve sustainable nutrition strategies. Sugar reduction and plant-based diets are two major focus areas of innovation in sustainable nutrition.
In this webinar, learn about:
-The science of flavour modulation and how it can help achieve sustainable nutrition goals
-How flavour modulation can account for taste and mouthfeel challenges in reduced sugar applications
-Strategies to understand and account for unique challenges of different plant protein sources
-How to bring this science to life in examples from the beverage market
Sustainable nutrition: sugar reduction
Producing one kilogram of sugar cane requires 1,110 litres of water and results in 0.42kg of CO2 emissions. This means that sugar reduction is not just important for improving health, but is also important in developing products that are better for the planet.
However, reducing sugar affects not only the sweetness of a beverage, but also its mouthfeel. Alternative solutions to sugar often come with detectable flavour off-notes. Learning how to account for each of these challenges in sugar reduction is essential to meeting the taste expectations of consumers.
Sustainable nutrition: plant proteins
The popularity of plant-based diets and use of plant protein is continually rising, leading to tremendous growth in markets like alternative dairy. This is both due to the health halo of plant-based foods, as well as the positive impact plant-based diets can have on the environment.
Different types of plant proteins are entering the market daily, but each plant protein comes with unique taste and mouthfeel challenges depending on the plant from which they are derived, where they’re grown, and how they’re processed. Understanding the science of accounting for challenges specific to each ingredient being used can be a great advantage in product development.
Identifying ingredients that have nutrition value from existing waste streams is one way to make strides toward a more circular economy with regards to sustainable nutrition.
Brewery spent grains are the most abundant by-product of the brewing industry, mainly used as animal feed in current food systems. Brewery spent grains are rich in fiber, protein, and phenolic compounds, making them a potential candidate for upcycling into nutrition ingredients in the human food supply.

A recent study published in the Journal of Food Science measured the impact that nutrition and sustainability messaging had on consumer purchase intent for cereal bars using brewery spent grains as an ingredient. The bars contained 12% brewery spent grains and were tested against commercial cereal bars.
Sustainability and nutrition messaging had a positive effect
The cereal bar made with brewery spent grains was perceived as natural by a significantly higher number of panelists (49%) compared to the control product. Calling out the fiber content of the product had a positive impact on purchase intent, as did calling out the use of upcycled ingredients. For these panelists, the sustainability messaging had a larger impact on purchase intent than the nutrition messaging.
Overcoming taste challenges will be important for upcycled ingredients
The commercial cereal bar outperformed the bar formulated with brewery spent grains in most measures for sensory attributes and liking. This finding has a couple of implications. First, the finding that sustainability and nutrition messaging on the product still improved purchase intent for the product with brewery spent grains shows that consumers are willing to forgive some changes in taste. Second, it shows the importance of understanding the properties of upcycled ingredients, each of which will pose different challenges for taste and formulation.
High moisture levels pose a hurdle for upcycling spent grains
Interest in upcycling spent grains into the human food supply has been building for years due to its promising nutrient content. However, a main challenge is the high moisture content of this brewing by-product. Spent grain can be up to 70-80% water by weight, which poses a challenge for transportation costs due to the weight of water.
The high moisture content, combined with the nutrients found in spent grains, gives microbes an environment that encourages growth. This can lead to fast spoilage and potentially pose a foodbourne illness risk. These reasons are why spent grains have been mainly limited to being used as animal feed in locations local to the brewery in which they were created.
Methods that can reduce the risk of spoilage or growth of pathogenic bacteria, without addition of ingredients that would take away from the natural appeal of using an upcycled ingredient in food, will be key for using spent grains in the human food supply at a global level.
Implications of the study
Overall, this study showed that consumers desire seeing information about both nutrition and sustainability on a package. Although the participants of this study still had high purchase intent despite lower taste and sensory performance, another takeaway is that a product that is optimized for taste, sustainability, and nutrition can maximize appeal.
A link to the study can be found here: Impact of sustainability and nutritional messaging on Italian consumers’ purchase intent of cereal bars made with brewery spent grains
In this webinar, learn:
- How we can optimize plant based protein for taste and nutrition – what we do and don’t know about healthy diets and the role of protein sources
- How we can optimize new plant-based proteins for the environment – highlighting the trade-offs and unknowns of plant-based protein development
- Which new protein sources have the most promise? – addressing the limitations of a few ‘hot’ sources and highlighting a few under-explored but high-potential options
Plant-based alternatives are perceived as being a healthier and more environmentally friendly protein source and can play a key role in reducing the environmental footprint of food production systems. However, this should not overshadow that the over-reliance on a limited number of crops can cause issues such as water scarcity, deforestation and biodiversity loss in some parts of the world.
Plant-based protein can provide complete amino acid nutrition when consumed as part of a balanced diet. As plant-based foods are introduced as snacks or indulgence foods, there is a need for transparency in their health credentials – products which are highly refined, or high in fat, sugar, salt or artificial preservatives may not retain the benefits of eating plant-based.
The above issues are key considerations to ensure the hoped-for potential of a plant-based future, can indeed, become a reality.
Is dairy fat healthy or unhealthy?
Why do we see recommendations to reduce saturated fat intake, while at the same time see headlines from studies showing full-fat dairy may be healthy for us?
The answer lies in the fact that food can often be more than the sum of its parts.
Dairy, saturated fat & health
Dairy is a nutrient rich food group which has been championed for its role in bone, dental and muscle health for decades. On the contrary, dairy has also been the subject of ‘negative press’ concerning its saturated fat content, which is linked to heart disease and other metabolic complications. Cardiovascular disease (CVD) remains the number 1 cause of mortality globally, representing 31% of all deaths (1).
The effect of saturated fat on health has been hotly debated in recent years and the latest evidence review for Saturated Fat and Health from the UK Scientific Advisory Committee on Nutrition (August 1st, 2019) recommends limiting saturated fat intake to ~10% of total calories (2). Saturated fat raises blood cholesterol levels, particularly low-density lipoprotein (LDL) cholesterol, which is a primary risk factor for cardiovascular disease.
At the same time, recent evidence from several large prospective cohort studies, systematic reviews and meta-analyses combining the results of thousands of subjects, have shown that milk and dairy foods, which can be high in saturated fat, have neutral or protective effects on cardiometabolic diseases (3-6).

These studies are having an impact on people’s beliefs of dairy. The idea that dairy fat is healthy is becoming more widespread among consumers. Bulletproof coffee, which encourages adding dairy fat to coffee specifically for potential health benefits, has grown into a successful lifestyle brand, and full-fat dairy is often encouraged as part of the ketogenic diet, one of the most popular diets in the world.
Whole milk and yoghurt have a saturated fat content of 2.3%, however cheese can range from 3-35% saturated fat which means that dairy is often targeted by public health bodies in efforts to reduce saturated fat intake. However, recent evidence has shown that cheese consumption does not raise LDL cholesterol compared to the same amount of fat from butter (7). This paradox may be due to a theory known as the ‘Dairy Matrix’. In reality, we eat whole foods rather than single nutrients. Dietary recommendations to reduce saturated fat do not distinguish between nutritionally poor ‘fried processed foods’ and nutritionally dense foods such as dairy.
How can a food high in saturated fat be healthy?
The Dairy Matrix: more than the sum of its parts
Dairy is a unique blend of nutrients including calcium, phosphorus, iodine, Vitamin B2 and B12, fermented cultures (yoghurt and cheese) bioactive peptides and high-quality protein containing all of the essential amino acids. Recently, scientists are considering the effects of milk and dairy foods on health beyond the benefits of the individual nutrients they contain. ‘The Dairy Matrix’ hypothesis suggests that the nutrients in dairy can interact with one another in ways that are beneficial for health (8).
Studies show that the dairy matrix has health benefits beyond the individual supplementation of the same nutrients and effective on cardiometabolic disease, weight management, bone mass density, bone metabolism, blood lipid levels and blood pressure (9).
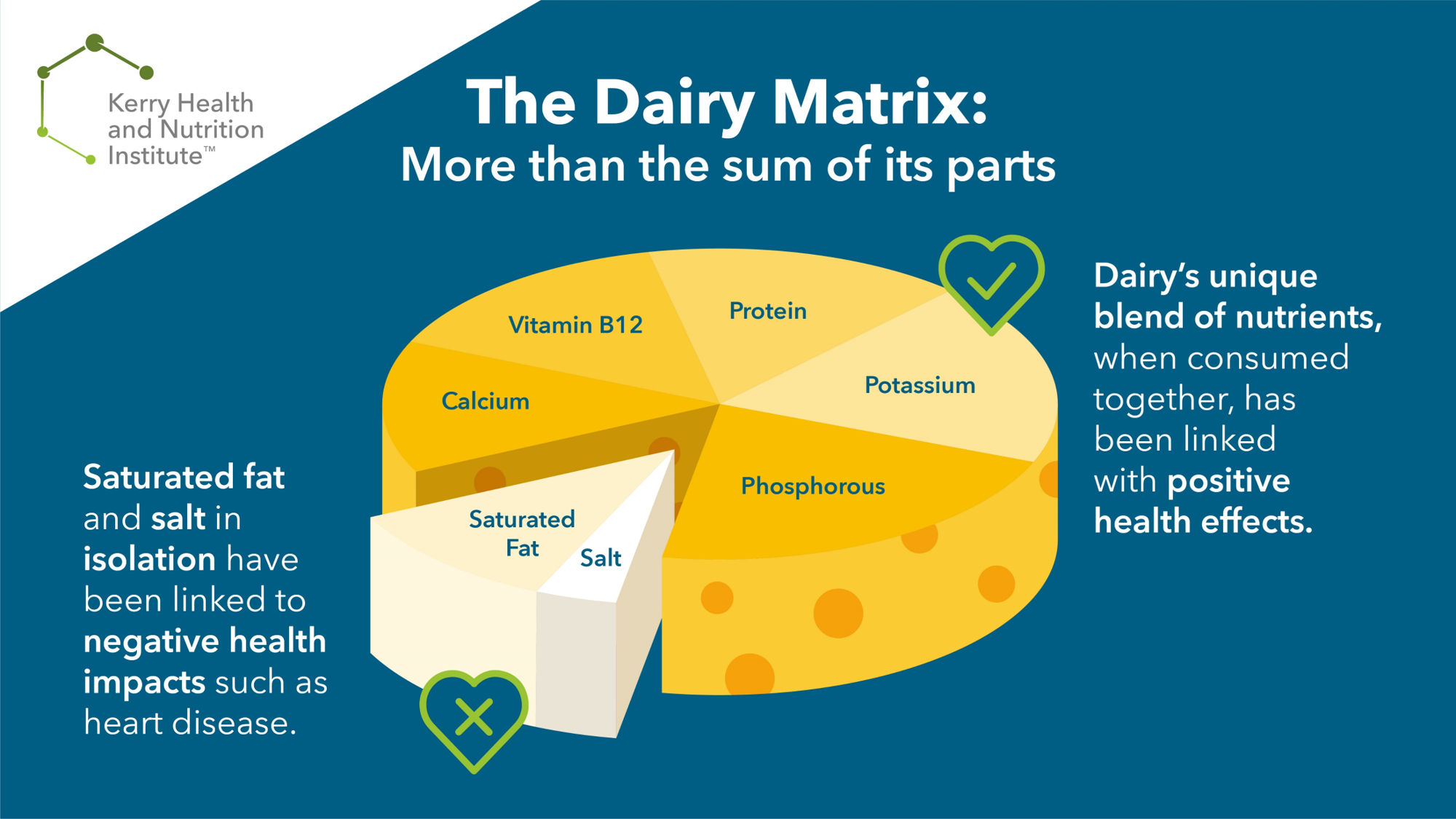
Is cheese good or bad for heart health?
In relation to cheese, the explanation for the beneficial rather than harmful effects on cardiovascular diseases (CVD) might be due to interactions between components of the cheese matrix, including calcium, phosphorus, the milkfat globule membrane, and starter cultures, which together modify saturated fatty acid-induced increases in blood lipids. One thought is that these nutrients may block absorption of the saturated fats in cheese, but this has not been proven.
A 2018 study published in the American Journal of Clinical Nutrition examined the effects of dairy fat in cheese versus butter on markers of cardiometabolic health in 164 overweight volunteers. They consumed 40g dairy fat daily for 6 weeks, one group consumed the fat as cheddar cheese and another group consumed the fat as butter (matched for calcium and protein). Results indicated that dairy fat, eaten in the form of cheese, appears to differently affect blood lipids compared with the same constituents eaten in a butter matrix, with significantly lower total cholesterol observed when all nutrients are consumed within a cheese matrix (10). Observational studies have also shown that yoghurt and cheese consumption are linked to a reduce risk of diabetes (6, 8).
Dairy and bone health: more than just calcium?
Furthermore, the effects of milk and dairy foods on bone health may be due in part to positive interactions of calcium, protein and phosphorus with each other and with lactose and bioactive peptides in the dairy matrices, rather than simply a ‘calcium effect’ as is often assumed (11). Similarly, milk is a key element of the Dietary Approaches to Stop Hypertension (DASH) diet for preventing and treating blood pressure. This anti-hypertensive property is likely due to the combination of minerals and protein found in dairy. Moreover, a study examining the effects of cows’ milk, calcium fortified soy milk and calcium supplement on weight and body fat reduction in premenopausal overweight and obese women found that weight loss was greatest in subjects consuming milk compared to calcium matched soy drink and calcium supplements (12).

Emerging research on the dairy matrix and health
- Bioactive peptides present in milk are being investigated in relation to cardiometabolic health, immune health and (13).
- Fermented dairy contains bacteria with potential to produce short chain fatty acids in the gut which can have positive health benefits (14).
- Dairy fat has >400 fatty acids with different physiological properties. Milk fat globule membrane (MFGM) encloses the fatty acids and has shown potential benefits in relation to lipid metabolism (15)
- Dairy fat contains odd chain fatty acids C15 and C17 which cannot be synthesised by the body and are used as biomarkers of dairy intake. These fatty acids are contained in MFGM and may confer health benefits such as reduced risk of CVD and Type 2 Diabetes (16-17)
- Grass fed dairy products have higher levels of polyunsaturated fat Conjugated Linoleic acid which has shown potential benefits for cardiometabolic health. See link to our article about the Nutrition Benefits of Grass fed dairy.
- Food is complex in terms of its nutritional content and physical structure which can impact the digestion and metabolism of the nutrients. The structure of dairy products varies from the solid matrix of cheese, to the gel-like structure of yogurt, to liquid milk. Rates of gastric emptying can affect satiety and appetite.
- The matrix structure can also influence protein absorption. Casein consumed in a milk matrix is more slowly digested and absorbed than in supplement format, without an impact on muscle protein synthesis (18).
More research into the dairy matrix will allow us to fully understand the health benefits of dairy but current evidence indicates that dairy is a nutritious food group that contributes positively to overall health when eaten as part of a balanced diet.
In recent years, many people are choosing to reduce /remove dairy from their diet due to a variety of reasons such as veganism, taste preferences, intolerance, to promote animal welfare and environmental sustainability. However, removing dairy from the diet should be carefully considered as it is a major source of nutrients and significant efforts should be made to ensure the diet is nutritionally balanced. A registered Dietitian or Nutritionist can support with individualised advice for meeting dietary requirements.
 Plant-based diets are becoming increasingly popular, but not all sources of nutrients are the same. Animal-based foods like milk or meat are rich sources of certain essential nutrients that are easily absorbed by the human body. These same nutrients are present in many plants but can sometimes be less available to the human body to digest and absorb. Therefore, nutrient bioavailability must be considered when consuming a plant-based diet. Many factors can affect nutrient bioavailability such as anti-nutrients[1] like oxalates, phytates, and tannins; cooking and processing methods; and factors in the human body
Plant-based diets are becoming increasingly popular, but not all sources of nutrients are the same. Animal-based foods like milk or meat are rich sources of certain essential nutrients that are easily absorbed by the human body. These same nutrients are present in many plants but can sometimes be less available to the human body to digest and absorb. Therefore, nutrient bioavailability must be considered when consuming a plant-based diet. Many factors can affect nutrient bioavailability such as anti-nutrients[1] like oxalates, phytates, and tannins; cooking and processing methods; and factors in the human body
This science review looks at:
- Nutrients commonly under-consumed from a plant-based diet, and how to increase intake of those nutrients from plants
- Which nutrients are less bioavailable from plant-based foods
- How bioavailability can be improved by cooking and processing
The nutrients of special concern in plant-based diets are (click to jump to that nutrient on the page):
What does bioavailability mean?
The European Food Information Council (EUFIC) defines bioavailability as “the proportion of a nutrient that is absorbed from the diet and used for normal body functions”[2]. Everything food that is eaten needs to be digested and absorbed in the intestine, and the presence of some compounds in plants can make that process more difficult for the body. For example, antinutrients can block digestive enzymes from reaching parts of a food to be digested. Oxalic acid is a molecule that plants produce to bind extra calcium within the plant. This molecule helps the plant function properly, but it also means that when we eat the plant, the calcium is harder for the human body to digest and absorb. In this example, the calcium would have a low bioavailability.

Calcium
Plant-based calcium sources
Plant sources that are naturally rich in bioavailable calcium are limited[3],[4]. Commonly recommended plant sources of calcium include kale, legumes, figs, bok choy, and broccoli. However, the quantity and bioavailability of calcium within these foods is far lower than dairy products or calcium fortified foods[5],[6]. For example, the EPIC-Oxford cohort observed that vegans had inadequate intakes of calcium, approximately half the mean intake level of non-vegetarians[7]. The presence of oxalic acid, or oxalate, reduces calcium bioavailability[8]. Oxalic acid, which is present in many calcium rich plant foods, particularly leafy vegetables[9], binds to calcium to form oxalate, which is not very well absorbed across the gut[10].
Spinach is a renowned example of a food high in calcium, yet absorption is very low due to the oxalate content. Turnip greens have a similar calcium level but lower oxalate content, thus absorption is significantly higher than from spinach[11]. Grains and legumes, which in general make up a substantial part of a plant-based diet, are high in phytates, which bind calcium strongly and these complexes are insoluble in the small intestine, making them hard to digest and absorb. It is estimated that 32% of calcium from dairy-based foods is absorbed, but only 5% of calcium from spinach is absorbed.

|
Get KHNI articles delivered to your inbox
|
Improving bioavailability of plant-based calcium
Studies have shown reducing phytates levels significantly increases calcium absorption from grains, pulses and legumes[12],[13]. Tannins and fibre can also negatively affect calcium bioavailability. In vitro tests have shown that germinating and de-hulling cowpeas, lentils or chickpeas to reduce tannin and fibre levels can significantly increase calcium bioavailability[14].
Factors in the human body can also influence calcium bioavailability. Calcium is absorbed across the gut by vitamin D dependent active transport and facilitated diffusion. Therefore, an individual’s vitamin D levels can affect calcium absorption. Factors such as sex, age, and individual calcium stores affect the rate of facilitated diffusion. The lower a person’s calcium stores, the more the gut will absorb this nutrient, but this ability decreases with age[15].
To summarise, bioavailability of calcium in a plant-based diet is not optimum mainly due to the quantity and presence of innate inhibitors. Cooking or processing plants to remove antinutrients can improve bioavailability, and some plant-based sources of calcium are more bioavailable than others. However, it is commonly suggested that people who do not consume animal products, particularly dairy, should eat foods fortified with calcium or take a calcium and vitamin D supplement to meet the recommended daily allowance (RDA) for this mineral[16],[17].
Protein
Differences between plant-based protein and animal-based protein
The most obvious concern regarding protein in plant-based diets is that sources are generally limited in one or more essential amino acids that cannot be made by the human body. Therefore, plant-sourced proteins are often referred to as ‘incomplete’. This is contrary to animal derived protein sources, which contain complete combinations of essential amino acids. The most common limited essential amino acids in plant-based diets are lysine (mainly limited in cereals), methionine (legumes, nuts and seeds), tryptophan (cereals) and cysteine (legumes)[18].
Protein complementation
Protein complementation, the combination of vegetable proteins to get all of the amino acids that are essential for the body, is the most effective way to meet protein needs when consuming a plant-based diet[19]. Individuals who eat a variety of plant protein sources such as legumes, nuts, grains, and seeds in enough quantities can meet optimum protein needs through plant sources alone. Interestingly, protein complementation is not required for each meal, as the body has the capability of storing amino acids[20],[21].
Table 1. Examples of Protein Complementation[22],[23]
| Food | Limited Amino Acid | Complement |
| Grains
(Oat, Brown Rice, Wheat) |
Lysine, Threonine | Legumes
(e.g. Soy, Pea, Lentils, Beans) |
| Nuts and Seeds | Lysine | Legumes
(e.g. Soy, Pea, Lentils, Beans) |
| Legumes
(e.g. Soy, Pea, Lentils, Beans) |
Methionine | Brown Rice, Wheat, Potato |
| Corn | Tryptophan | Legumes
(e.g. Soy, Pea, Lentils, Beans) |
However, the amino acid content is not the only limitation to plant protein bioavailability. The presence of other components such as fibre, tannins, and phytates can reduce protein digestibility, thus making it more difficult for the body to utilise the amino acids.
Vitamin D
Sources of vitamin D
The human body acquires vitamin D by two methods: (1) vitamin D is produced in the skin via UV rays from sunlight and (2) intake from the diet. There are two forms of vitamin D: vitamin D3 (active form) and vitamin D2. Vitamin D3 is considerably more bioavailable than the plant source vitamin D2, which means vitamin D3 is more effective than vitamin D2 at raising serum 25(OH)D concentrations, which is an important molecule for the body to actively absorb calcium[24]. Vitamin D3 is produced by human skin in the presence of ultraviolet light from the sun, or sourced from animal products are rich in vitamin D3, whereas plant sources contain vitamin D2 only[25],[26].
Vitamin D levels of vegans and non-vegetarians
The EPIC-Oxford cohort reported the average vitamin D intakes of vegans were approximately 73% lower than non-vegetarians[27]. Vitamin D deficiency is evident within the European population at concerning rates of prevalence[28]. Recent national UK surveys identified 1 in 5 people with low vitamin D levels (serum levels below 25 nmol/L)[29]. Individuals that derive vitamin D from sunlight and a plant-based diet alone will unlikely meet the RDA for vitamin D, especially during winter. The Scientific Advisory Committee on Nutrition (SACN) advises to consume fortified foods and supplements to meet adequate vitamin D requirements[30]. More recently, England’s national health service (NHS) extended their recommendation of taking a daily supplement containing 10 micrograms vitamin D to the entire UK population. This is to counteract the risk of getting less sun exposure due to current measures enforced by UK government to keep people in their homes to control the spread of Covid-19[31].
Iron
The World Health Organisation (WHO) describes iron deficiency as the most common and widespread nutritional disorder in the world[32]. It is prevalent in developing countries where diets are predominantly plant-based. Deficiency is a major issue due to a significant amount of the population having high iron needs such as women of childbearing age, combined with the low bioavailability of iron in available foods.
Haem iron and non-haem iron
Iron is present in two forms: haem and non-haem iron. Haem iron is more readily absorbed across the gut compared to non-haem iron[33]. Red meat and other animal derived foods are rich sources of haem iron[34]. Plant sources contain non-haem iron only[35] and include foods such as green leafy vegetables, legumes, nuts, seeds, and grains.
Iron bioavailability can vary significantly due to inhibitors within the same or other foods in a meal[36]. Phytates, which are complexes found in legumes, grains, oil seeds and nuts, are arguably the most potent inhibitors to non-haem iron absorption[37]. Phytates form insoluble complexes in the gut, reducing iron bioavailability considerably[38].
Increasing iron bioavailability

Many studies have shown that common cooking and preparation methods such as fermenting, germinating and de-hulling legumes, and malting cereals can reduce phytate levels and, hence, increase iron bioavailability from these foods[39]. Phenolic compounds such as tannins and polyphenols, which are abundant in tea and coffee, also inhibit iron absorption. Avoiding drinking tea and coffee within two hours of consuming a meal rich in iron is recommended for individuals with low iron status[40],[41],[42].
Nutrient-nutrient interactions can also affect bioavailability. For instance, calcium is another inhibitor of iron bioavailability, due to competition for absorption across the intestinal wall. This is more often observed when calcium and iron are part of the same meal and calcium quantity is high[43].
On the other hand, foods rich in vitamin C can increase plant-based iron absorption[44] because this vitamin binds to non-haem iron to form a chelate that is soluble and digestible within the small intestine. However, it is important to note that cooking vitamin C-rich foods at a high temperature can destroy some of the vitamin C present in foods, reducing its ability to improve iron absorption[45],[46].
There is evidence to suggest individuals can maintain adequate iron stores without consuming animal derived foods, provided effective planning of meals to reduce the presence of inhibitors and increase enhancers is applied[47],[48]. This approach takes careful management, and the prevalence of iron deficiency globally would suggest fortification and supplementation are supported, especially for menstruating women[49].
Zinc
Zinc deficiency is prevalent globally, particularly for developing countries that consume a primarily plant-based diet[50]. This is mainly due to the low bioavailability of zinc in plant foods rather than a lack of plant zinc sources[51]. The EPIC-Oxford cohort reported that average zinc intakes of vegans were approximately 20% lower than non-vegetarians[52]. In this study, even non-vegetarians had zinc intakes that were below the RDA, suggesting that plant-based eaters might be at an even higher risk of deficiency due to the low bioavailability of plant-based zinc[53]. However, the American Dietetic Association and Dietitians of Canada expressed no considerable concern for vegetarians and inadequate zinc intakes in their position paper on vegetarian diets in 2003[54].
Plant-based zinc bioavailability
In research studies, zinc bioavailability from plant-based diets is often measured alongside iron. In general, good quality plant-based diets predominantly consist of whole grains and legumes, which are rich sources of zinc. As with non-haem iron, phytic acid has a significant inhibitory effect on zinc absorption[55],[56]. However, processing methods that can increase the activity of phytate degrading enzymes counteract this considerably. Processes such as heating, germination, soaking, and fermentation of legumes and grains increase zinc bioavailability, provided the optimum pH is achieved. Enzymes for degrading phytates work best in an acidic pH environment for cereals and neutral or alkaline for some legumes[57]. The high fibre content in whole grains and legumes inhibit zinc absorption but preparation methods like de-hulling, pressure-cooking, and fermentation can breakdown the fibre and enhance zinc bioavailability[58],[59].

There are studies suggesting that consuming a meal that is both high in protein and zinc has a positive effect on zinc bioavailability[60],[61],[62]. Although bioavailability of zinc in plant-based diets is low, with prudent cooking and meal planning, it is possible to meet adequate body needs.
Vitamin B12
The main dietary sources of Vitamin B12 are products derived from ruminants, such as cows, because microorganisms present in the digestive tracts of ruminants produce this nutrient[63]. Vitamin B12 is generally not present in plant foods, but fortified breakfast cereals are a readily available source of vitamin B12 with high bioavailability for vegetarians. This aligns with the EPIC-Oxford cohort observation that on average vegans consumed approximately 93% less vitamin B12 than meat eaters[64]. However, inadequate vitamin B12 quantities in plant-based diets are widely acknowledged and individuals following a plant-based diet are advised to consume foods fortified with vitamin B12 and to take a supplement[65],[66],[67].
Vitamin B12 absorption depends on two compounds produced in the stomach: (i) a protein called “intrinsic factor” (IF) and (ii) gastric acid. The ability of the stomach to produce these compounds functionality declines with age, thus the ability to absorb vitamin B12 reduces over time[68].
Vitamin B12 is typically added to foods and supplements in its free form, meaning gastric acid is not required to make this type of vitamin B12 absorbable. However, the IF is at capacity at only 1-2 mcg vitamin B12, and absorption decreases considerably then[69]. Therefore, vitamin B12 is best absorbed in small quantities. To ensure adequate intake individuals following a plant-based diet should eat vitamin B12 fortified foods on more than one occasion throughout the day[70].
Vitamin A
Sources of vitamin A
Vitamin A deficiency is a major issue in developing counties. There are two forms of vitamin A available in the human diet; preformed vitamin A, for example retinol, and provitamin A carotenoids. Animal derived products such as liver, fish oils, milk, and eggs are rich in preformed vitamin A. Both provitamin A carotenoids and preformed vitamin A must be metabolised before use by the body[71]. The most abundant and efficiently converted carotenoid in plant-based diets is b-Carotene, and provides fruits and vegetables, such as mangos, oranges, carrots, and beetroot, with a yellow/orange/red colour[72]. Conversion of b-Carotene to retinol is not very efficient in the body; therefore, the daily requirement of b-Carotene is considerably higher than the RDA for vitamin A[73]. Hence, RDAs for vitamin A are given as retinol activity equivalents (RAE) to account for the different bioactivities of retinol and provitamin A carotenoids. One mcg RAE is equivalent to 1 mcg retinol and 12 mcg dietary beta-carotene[74].
Vitamin A bioavailability
However, a healthy plant-based diet is abundant in fruit and vegetables that are rich in b-Carotene. Therefore, meeting the required amount is feasible[75], unless part of a population that depends on a staple diet of poor vitamin A source grain, such as rice. Cooking methods can increase the bioavailability of carotenoids, particularly heating in a little fat/oil[76],[77] or adding acidulants or antioxidant spices such as lime, tamarind, onion or turmeric[78]. Although b-Carotene bioavailability is lower than vitamin A, this can be overcome with a varied diet of fruit and vegetables and specific cooking processes.
Essential Fatty Acids
Omega-6 and Omega-3 fatty acids are both essential for the human body, meaning they need to be consumed in the diet to support adequate amounts in the body. The long chain omega-3 fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are key nutrients for optimum health and development. They contribute to many functions in the body such as normal brain and eye development and maintenance of cardiovascular health[79]. Oily fish are the richest source of these fatty acids, while plant-based diets are low in these nutrients[80]. The current UK dietary recommendation for essential fatty acid intake is to eat at least two portions of fish a week, one of which should be oily[81]. For some individuals, fish may not be part of a plant-based diet; therefore, levels of these fatty acids are generally sub-optimal.
Plant-based sources of omega-3 fats
The body can convert a plant sourced omega-3 fatty acid, a-linoleic acid (ALA) to EPA and DHA, however the conversion efficacy is low[82]. Good quality plant-based diets are high in ALA. Rich sources include chia seeds, flaxseeds, hemp seeds, and rapeseed oil[83],[84]. However, bioavailability of ALA is reduced by the presence of the omega-6 fatty acid linoleic acid (LA), which is also abundant in plant-based foods. Sources of LA include sunflower oil, sesame oil, almonds, and cashews[85]. LA competes with ALA for enzymes needed to convert ALA to EPA and DHA[86]. Therefore, good quality plant-based diets will aim to have a ratio of 1:3 omega-6 to omega-3 fatty acids in the diet and avoid them within the same meal[87].

Protein, calcium, biotin, magnesium and zinc can increase ALA bioavailability[88],[89], and a good quality plant-based diet is sufficient in these nutrients. According to the American Dietetic Association, a sufficient intake of ALA in the diet is adequate to meet EPA and DHA needs; however, if an individual has increased needs or poor conversion then a direct source such as DHA-rich microalgae is advised[90]. EPA and DHA supplementation is a controversial topic, as there were concerns regarding the safety of over consumption, however the European Food Safety Authority (EFSA) has concluded 5g of long-chain omega-3 fatty acids raise no safety concerns for adults[91].
Iodine
Iodine is an essential trace element imperative for brain development, normal growth and metabolism[92]. Plant foods can be insufficient and unreliable iodine sources[93]. Adequate iodine intake is a concern for people who follow a plant-based diet. Iodised salt policies were implemented in various countries across the globe to eradicate deficiency. However, recommendations to reduce salt intake to support heart health also mean reducing iodine intake. Most salt used in packaged foods is not iodised.
Iodine in plant-based diets

In the United States, Ireland, UK, and most of Europe, the main source of iodine is from milk and milk products, followed by fish and meat. The high content in milk is a result of iodine addition in cow feed and iodine-containing disinfectants used during milking[94]. Therefore, it is important to note that vegetarians who swap dairy milk to a plant-based alternative may be at risk of inadequate iodine intake. Furthermore, a study conducted by the University of Surrey reported that organic milk was 42% lower in iodine than conventional milk[95].
Seaweed is a very rich source of iodine, particularly kelp. However, the iodine content can be too high, and excessive iodine intake can have negative health effects. For this reason, it is advised to limit seaweed consumption to once a week, particularly if you are pregnant[96]. There is limited research investigating the bioavailability of iodine in plant-based diets, although it appears to be high[97]. However, most literature papers investigating vegan diets highlight iodine as a nutrient at risk of inadequate intakes[98],[99],[100].
Summary of Bioavailability for Plant-based Nutrients
Conclusion
Plant sources of certain nutrients have a significantly lower quantity and bioavailability compared with animal derived foods. Many factors can affect nutrient bioavailability including the presence of anti-nutrients; cooking and processing methods; host factors; and nutrient-nutrient interactions. Bioavailability is an important factor when evaluating the quality of a diet because it has a substantial effect on the amount of nutrients available to the body for important functions. Therefore, rating foods and diets on nutrient quantities alone is not fully reflective of nutritional quality.
It is important to note that plant-based diets can meet the nutritional needs of an individual, provided they are good quality and supplemented with specific nutrients, if needed[101] [102].
References
[1] Ghavidel R A, Prakash J. The impact of germination and dehulling on nutrients, antinutrients, in vitro iron and calcium bioavailability and in vitro starch and protein digestibility of some legume seeds. LWT – Food Science and Technology. 2007 Sep; 40(7):1292-1299.
[2] The European Food Information Council (2010) ‘Nutrient bioavailability: Getting the most out of food’ https://www.eufic.org/en/food-today/article/nutrient-bioavailability-getting-the-most-out-of-food. Accessed May 2020.
[3] Yang J, Punshon T, Guerinot M, et al. (2012) ‘Plant Calcium Content: Ready to Remode.’ Nutrients. 2012 Aug; 4(8): 1120–1136. Published online 2012 Aug 21. doi: 10.3390/nu4081120
[4] Clarys P, Deliens T, Huybrechts I, et al. (2014) ‘Comparison of nutritional quality of the vegan, vegetarian, semi-vegetarian, pesco-vegetarian and omnivorous diet.’ Nutrients. 2014 Mar 24; 6(3):1318-32.
[5] Messina V, Mangels AR. (2001) ‘Considerations in planning vegan diets: children.’ J Am Diet Assoc. 2001 Jun;101(6):661-9.
[6] Platel K, Srinivasan K. (2013) ‘Bioavailability of Micronutrients from Plant Foods: An Update.’ Crit Rev Food Sci Nutr. 2016 Jul 26;56(10):1608-19. doi: 10.1080/10408398.2013.781011.
[7] Davey GK, Spencer EA, Appleby PN, et al. (2003) ’EPIC-Oxford: lifestyle characteristics and nutrient intakes in a cohort of 33 883 meat-eaters and 31 546 non meat-eaters in the UK.’ Public Health Nutr. 2003 May;6(3):259-69.
[8] Amalraj A, Pius A.(2015) ‘Bioavailability of calcium and its absorption inhibitors in raw and cooked green leafy vegetables commonly consumed in India – An in vitro study.’ Food Chemistry. (2015) Mar 1;170:430-6. doi: 10.1016/j.foodchem.2014.08.031. Epub 2014 Aug 27.
[9] Noonan SC, Savage GP. (1999) ‘Oxalate content of foods and its effect on humans.’ Asia Pacific J Clin Nutr. (1999) 8(1): 64-74
[10] Yang, Jian et al. “Plant calcium content: ready to remodel.” Nutrients vol. 4,8 (2012): 1120-36. doi:10.3390/nu4081120
[11] Cockwell KA. Calcium. Elsevier Science Ltd., 2003.
[12] Ghavidel R A, Prakash J. The impact of germination and dehulling on nutrients, antinutrients, in vitro iron and calcium bioavailability and in vitro starch and protein digestibility of some legume seeds. LWT – Food Science and Technology. 2007 Sep; 40(7):1292-1299.
[13] Hambidge KM, Krebs NF, Westcott JL, et al. (2005) ‘Absorption of calcium from tortilla meals prepared from low-phytate maize.’ Am J Clin Nutr. 2005 Jul;82(1):84-7.
[14] Ghavidel R A, Prakash J. The impact of germination and dehulling on nutrients, antinutrients, in vitro iron and calcium bioavailability and in vitro starch and protein digestibility of some legume seeds. LWT – Food Science and Technology. 2007 Sep; 40(7):1292-1299.
[15] Caroli A et al. (2011) ‘Invited review: Dairy intake and bone health: A viewpoint from the state of the art.’ J Dairy Sci 2011;94(11):5249-62.
[16] Craig WJ. (2009) ‘Health effects of vegan diets.’ Am J Clin Nutr. 2009;89(5):1627S–1633S. doi: 10.3945/ajcn.2009.26736N.
[17] American Dietetic Association; Dietitians of Canada. (2003) ‘Position of the American Dietetic Association and Dietitians of Canada: Vegetarian diets.’ J Am Diet Assoc. 2003 Jun;103(6):748-65.
[18] Lonnie, Marta et al. “Protein for Life: Review of Optimal Protein Intake, Sustainable Dietary Sources and the Effect on Appetite in Ageing Adults.” Nutrients vol. 10,3 360. 16 Mar. 2018, doi:10.3390/nu10030360
[19] American Society for Nutrition. (2011) “Community and Public Health Nutrition; Protein Complementation”. https://nutrition.org/protein-complementation/. Accessed May 2020.
[20] American Dietetic Association; Dietitians of Canada. (2003) ‘Position of the American Dietetic Association and Dietitians of Canada: Vegetarian diets.’ J Am Diet Assoc. 2003 Jun;103(6):748-65.
[21] De Gavelle, Erwan et al. “Protein Adequacy Is Primarily a Matter of Protein Quantity, Not Quality: Modeling an Increase in Plant:Animal Protein Ratio in French Adults.” Nutrients vol. 9,12 1333. 8 Dec. 2017, doi:10.3390/nu9121333
[22] American Society for Nutrition. (2011) “Community and Public Health Nutrition; Protein Complementation”. https://nutrition.org/protein-complementation/. Accessed May 2020.
[23] Jonnalagadda S. Matthews O. (2020) ‘Nutritional Benefits of Plant Proteins Taking Root with Consumers’. Kerry health and Nutrition Institute. https://khni.kerry.com/news/blog/nutritional-benefits-of-plant-proteins-taking-root-with-consumers/. Accessed: May 2020.
[24] Trang HM, Cole DE, Rubin LA, et al. (1998) Evidence that vitamin D3 increases serum 25-hydroxyvitamin D more efficiently than does vitamin D2. Am J Clin Nutr. 1998 Oct;68(4):854-8.
[25] Nair, R., & Maseeh, A. (2012). Vitamin D: The “sunshine” vitamin. Journal of pharmacology & pharmacotherapeutics, 3(2), 118–126. https://doi.org/10.4103/0976-500X.95506
[26] NHS. (2020) ‘Vitamins and Minerals; Vitamin D’ https://www.nhs.uk/conditions/vitamins-and-minerals/vitamin-d/. Accessed: May 2020
[27] Davey GK, Spencer EA, Appleby PN, et al. (2003) ‘EPIC-Oxford: lifestyle characteristics and nutrient intakes in a cohort of 33 883 meat-eaters and 31 546 non meat-eaters in the UK.’ Public Health Nutr. 2003 May;6(3):259-69.
[28] Cashman, Kevin D et al. “Vitamin D deficiency in Europe: pandemic?.” The American journal of clinical nutrition vol. 103,4 (2016): 1033-44. doi:10.3945/ajcn.115.120873
[29] British Nutrition Foundation. (2020) ‘New advice on Vitamin D.’ British Nutrition Foundation website. https://www.nutrition.org.uk/nutritioninthenews/new-reports/983-newvitamind.html. Accessed: May 2020.
[30] The Scientific Advisory Committee on Nutrition (SACN) (2016) ‘Vitamin D and Health’. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/537616/SACN_Vitamin_D_and_Health_report.pdf. Accessed: May 2020.
[31] NHS. (2020) ‘Vitamins and Minerals; Vitamin D’ https://www.nhs.uk/conditions/vitamins-and-minerals/vitamin-d/. Accessed: May 2020
[32] De Benoist, Hempstead R. (2001). ‘Iron Deficiency Anaemia Assessment, Prevention and Control A guide for programme managers’ World Health Organisation’ 2001 5(15).
[33] West, A. R., & Oates, P. S. (2008). Mechanisms of heme iron absorption: current questions and controversies. World journal of gastroenterology, 14(26), 4101–4110. https://doi.org/10.3748/wjg.14.4101
[34] Young, I., Parker, H. M., Rangan, A., et al. (2018). ‘Association between Haem and Non-Haem Iron Intake and Serum Ferritin in Healthy Young Women.’ Nutrients, 10(1), 81. https://doi.org/10.3390/nu10010081
[35] American Dietetic Association; Dietitians of Canada. (2003) ‘Position of the American Dietetic Association and Dietitians of Canada: Vegetarian diets.’ J Am Diet Assoc. 2003 Jun;103(6):748-65.
[36] Sandberg AS. (2002) Bioavailability of minerals in legumes.Br J Nutr. 2002 Dec;88 Suppl 3:S281-5.
[37] Gupta, Raj Kishor et al. (2015) “Reduction of phytic acid and enhancement of bioavailable micronutrients in food grains.” Journal of food science and technology 2015;52(2):676‐684. doi:10.1007/s13197-013-0978-y
[38] Sandberg AS. (2002) Bioavailability of minerals in legumes.Br J Nutr. 2002 Dec;88 Suppl 3:S281-5.
[39] Gibson RS, Perlas L, Hotz C. (2006) Improving the bioavailability of nutrients in plant foods at the household level. Proceedings of the Nutrition Society (2006), 65, 160–168 Proceedings of the Nutrition Society (2006), 65, 160–168 DOI:10.1079/PNS2006489
[40] De Benoist, Hempstead R. (2001). ‘Iron Deficiency Anaemia Assessment, Prevention and Control A guide for programme managers’ World Health Organisation’ 2001 8(66).
[41] Janet R, Hunt Am. (2003) ‘Bioavailability of iron, zinc, and other trace minerals from
vegetarian diet.’ J Clin Nutr 2003;78(suppl):633S–9S
[42] Delimont NM, Haub MD, Lindshield BL. (2017) ‘The Impact of Tannin Consumption on Iron Bioavailability and Status: A Narrative Review.’ Curr Dev Nutr. 2017 Feb; 1(2): 1–12. Published online 2017 Jan 19. doi: 10.3945/cdn.116.000042
[43] Hallberg L, Rossander-Hultén L, Brune M, Gleerup A. (1992) ‘Calcium and iron absorption: mechanism of action and nutritional importance.’ Eur J Clin Nutr. 1992;46(5):317‐327
[44] Purushothaman V, M A, Tsou SC, S S. Supplementing iron bioavailability enhanced mung bean. Asia Pac J Clin Nutr. 2008;17 Suppl 1:99-102.
[45] Teucher B, Olivares M, Cori H. (2004) ‘Enhancers of iron absorption: ascorbic acid and other organic acids.’ Int J Vitam Nutr Res. 2004;74(6):403‐419. doi:10.1024/0300-9831.74.6.403
[46] Lynch SR, Cook JD. (1980) ’Interaction of vitamin C and iron.’ Ann N Y Acad Sci. 1980;355:32‐44. doi:10.1111/j.1749-6632.1980.tb21325.x
[47] Young, I., Parker, H. M., Rangan, A., et al. (2018). ‘Association between Haem and Non-Haem Iron Intake and Serum Ferritin in Healthy Young Women.’ Nutrients, 10(1), 81. https://doi.org/10.3390/nu10010081
[48] Anderson BM, Gibson RS, Sabry JH. (1981) ‘The iron and zinc status of long-term vegetarian women.’ Am J Clin Nutr. 1981 Jun;34(6):1042-8
[49] De Benoist, Hempstead R. (2001). ‘Iron Deficiency Anaemia Assessment, Prevention and Control A guide for programme managers’ World Health Organisation’ 2001 8(66).
[50]IZiNCG Secretariat. UCSF Benioff Children’s Hospital Oakland. (2019) ‘ESTIMATING NATIONAL RISK OF ZINC DEFICIENCY: PROXY INDICATORS VS. PLASMA/SERUM ZINC CONCENTRATIONS’. https://www.izincg.org/new-blog-1/estimating-national-risk-of-zinc-deficiency
[51] Platel K, Srinivasan K. (2016) ‘Bioavailability of Micronutrients from Plant Foods: An Update.’ Crit Rev Food Sci Nutr. 2016 Jul 26;56(10):1608-19. doi: 10.1080/10408398.2013.781011.
[52] Davey GK, Spencer EA, Appleby PN, et al. (2003) ‘EPIC-Oxford: lifestyle characteristics and nutrient intakes in a cohort of 33 883 meat-eaters and 31 546 non meat-eaters in the UK.’ Public Health Nutr. 2003 May;6(3):259-69.
[53] Davey GK, Spencer EA, Appleby PN, et al. (2003) ‘EPIC-Oxford: lifestyle characteristics and nutrient intakes in a cohort of 33 883 meat-eaters and 31 546 non meat-eaters in the UK.’ Public Health Nutr. 2003 May;6(3):259-69.
[54] American Dietetic Association; Dietitians of Canada. (2003) ‘Position of the American Dietetic Association and Dietitians of Canada: Vegetarian diets.’ J Am Diet Assoc. 2003 Jun;103(6):748-65.
[55] Janet R, Hunt Am. (203) ‘Bioavailability of iron, zinc, and other trace minerals from
vegetarian diet.’ J Clin Nutr 2003;78(suppl):633S–9S
[56] Fredlund K, Isaksson M, Rossander-Hulthén L, et al. (2006) ‘Absorption of zinc and retention of calcium: dose-dependent inhibition by phytate.’ J Trace Elem Med Biol. 2006;20(1):49-57. Epub 2006 Mar 2.
[57] Sandberg AS. (2002) Bioavailability of minerals in legumes.Br J Nutr. 2002 Dec;88 Suppl 3:S281-5.
[58] Hemalatha, S., Platel, K. and Srinivasan, K. (2007). ‘Zinc and iron content and their bioaccessibility in cereals and pulses consumed in India.’ Food Chem. 102:1328–1336.
[59] Suliburska, J., & Krejpcio, Z. (2014). Evaluation of the content and bioaccessibility of iron, zinc, calcium and magnesium from groats, rice, leguminous grains and nuts. Journal of food science and technology, 51(3), 589–594. https://doi.org/10.1007/s13197-011-0535-5
[60] Dietary factors influencing zinc absorption. J Nutr. 2000 May;130(5S Suppl):1378S-83S. doi: 10.1093/jn/130.5.1378S.
[61] Platel K, Srinivasan K. (2016) ‘Bioavailability of Micronutrients from Plant Foods: An Update.’ Crit Rev Food Sci Nutr. 2016 Jul 26;56(10):1608-19. doi: 10.1080/10408398.2013.781011.
[62] Janet R, Hunt Am. (2003) ‘Bioavailability of iron, zinc, and other trace minerals from vegetarian diet.’ J Clin Nutr 2003;78(suppl):633S–9S
[63] Rogerson D. (2017) ‘Vegan diets: practical advice for athletes and exercisers.’ J Int Soc Sports Nutr. 2017; 14: 36. Published online 2017 Sep 13. doi: 10.1186/s12970-017-0192-
[64] Davey GK, Spencer EA, Appleby PN, et al. (2003) ‘EPIC-Oxford: lifestyle characteristics and nutrient intakes in a cohort of 33 883 meat-eaters and 31 546 non meat-eaters in the UK.’ Public Health Nutr. 2003 May;6(3):259-69.
[65] Davey GK, Spencer EA, Appleby PN, et al. (2003) ‘EPIC-Oxford: lifestyle characteristics and nutrient intakes in a cohort of 33 883 meat-eaters and 31 546 non meat-eaters in the UK.’ Public Health Nutr. 2003 May;6(3):259-69.
[66] Messina V, Mangels AR. (2001) ‘Considerations in planning vegan diets: children.’ J Am Diet Assoc. 2001 Jun;101(6):661-9.
[67] Craig WJ. (2009) ‘Health effects of vegan diets.’ Am J Clin Nutr. 2009;89(5):1627S–1633S. doi: 10.3945/ajcn.2009.26736N.
[68] Agnoli C, Baroni L, Bertini I, et al. (2017) ‘Position paper on vegetarian diets from the working group of the Italian Society of Human Nutrition.’ Nutr Metab Cardiovasc Dis. 2017 Dec;27(12):1037-1052. doi: 10.1016/j.numecd.2017.10.020. Epub 2017 Oct 31.
[69] Office of Dietary Supplements (February 2020) ‘Vitamin B12; Fact Sheet for Consumers’ U.S. Department of Health & Human Services; National Institutes of Health: https://ods.od.nih.gov/pdf/factsheets/VitaminB12-Consumer.pdf
[70] British Dietetic Association (2017) ‘Plant-based diet: Food Fact Sheet’. https://www.bda.uk.com/resource/plant-based-diet.html. Accessed: May 2020.
[71] Office of Dietary Supplements (March 2020) ‘Vitamin A; Fact Sheet for Health Professionals’ U.S. Department of Health & Human Services; National Institutes of Health:https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/#h3. Accessed on: May 2020.
[72] Platel K, Srinivasan K. (2013) ‘Bioavailability of Micronutrients from Plant Foods: An Update.’ Crit Rev Food Sci Nutr. 2016 Jul 26;56(10):1608-19. doi: 10.1080/10408398.2013.781011.
[73] Platel K, Srinivasan K. (2013) ‘Bioavailability of Micronutrients from Plant Foods: An Update.’ Crit Rev Food Sci Nutr. 2016 Jul 26;56(10):1608-19. doi: 10.1080/10408398.2013.781011.
[74] Office of Dietary Supplements (March 2020) ‘Vitamin A; Fact Sheet for Health Professionals’ U.S. Department of Health & Human Services; National Institutes of Health:https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional/#h3. Accessed on: May 2020.
[75] American Dietetic Association; Dietitians of Canada. (2003) ‘Position of the American Dietetic Association and Dietitians of Canada: Vegetarian diets.’ J Am Diet Assoc. 2003 Jun;103(6):748-65.
[76] American Dietetic Association; Dietitians of Canada. (2003) ‘Position of the American Dietetic Association and Dietitians of Canada: Vegetarian diets.’ J Am Diet Assoc. 2003 Jun;103(6):748-65.
[77] Nair K M, Augustine LF. (2018) ‘Food synergies for improving bioavailability of micronutrients from
plant foods’. Food Chemistry. 2018. 238:180–185.
[78] Veda S, Platel K, Srinivasan K.J.(2008) ‘Influence of food acidulants and antioxidant spices on the bioaccessibility of beta-carotene from selected vegetables.’ Agric Food Chem. 2008 Sep 24;56(18):8714-9. doi: 10.1021/jf801374d. Epub 2008 Aug 27.
[79]European Food Safety Authority (2020) ‘EU Register on nutrition and health claims.’ https://ec.europa.eu/food/safety/labelling_nutrition/claims/register/public/?event=search. Accessed May 2020.
[80] Agnoli C, Baroni L, Bertini I, et al. (2017) ‘Position paper on vegetarian diets from the working group of the Italian Society of Human Nutrition.’ Nutr Metab Cardiovasc Dis. 2017 Dec;27(12):1037-1052. doi: 10.1016/j.numecd.2017.10.020. Epub 2017 Oct 31.
[81] British Nutrition Foundation (2018) ‘The Eatwell Guide – A revised healthy eating model’. https://www.nutrition.org.uk/healthyliving/healthydiet/eatwell.html. Accessed May 2020.
[82] Rogerson D. (2017) ‘Vegan diets: practical advice for athletes and exercisers.’ J Int Soc Sports Nutr. 2017; 14: 36. Published online 2017 Sep 13. doi: 10.1186/s12970-017-0192-
[83] Agnoli C, Baroni L, Bertini I; et al. (2017) ‘Nutrition, Metabolism & Cardiovascular Diseases Position paper on vegetarian diets from the working group of the Italian Society of Human Nutrition.’ Nutr. Metab. Cardiovasc. Dis. 2017, 27, 1037–1052.
[84] Welch A, Shakya-Shrestha S, Lentjes M, et al. (2010) ‘Dietary intake and status of n-3 polyunsaturated fatty acids in a population of fish-eating and non fish-eating meat-eaters, vegetarians, and vegans and the precursor-product ratio of a-linolenic acid to long-chain n-3 polyunsaturated fatty acids: Results from the EPIC-Norfolk cohort.’ Am. J. Clin. Nutr. 2010, 92, 1040–1051
[85] Whelan, Jay, and Kevin Fritsche. (2013) “Linoleic acid.” Advances in nutrition (Bethesda, Md.) vol. 4,3 311-2. 1 May. 2013, doi:10.3945/an.113.003772
[86] Cholewski, Mateusz et al. (2018) “A Comprehensive Review of Chemistry, Sources and Bioavailability of Omega-3 Fatty Acids.” Nutrients vol. 10,11 1662. 4 Nov. 2018, doi:10.3390/nu10111662
[87] Welch A, Shakya-Shrestha S, Lentjes M, et al. (2010) ‘Dietary intake and status of n-3 polyunsaturated fatty acids in a population of fish-eating and non fish-eating meat-eaters, vegetarians, and vegans and the precursor-product ratio of a-linolenic acid to long-chain n-3 polyunsaturated fatty acids: Results from the EPIC-Norfolk cohort.’ Am. J. Clin. Nutr. 2010, 92, 1040–1051
[88] Welch A, Shakya-Shrestha S, Lentjes M, et al. (2010) ‘Dietary intake and status of n-3 polyunsaturated fatty acids in a population of fish-eating and non fish-eating meat-eaters, vegetarians, and vegans and the precursor-product ratio of a-linolenic acid to long-chain n-3 polyunsaturated fatty acids: Results from the EPIC-Norfolk cohort.’ Am. J. Clin. Nutr. 2010, 92, 1040–1051
[89] Rogerson D. (2017) ‘Vegan diets: practical advice for athletes and exercisers.’ J Int Soc Sports Nutr. 2017; 14: 36. Published online 2017 Sep 13. doi: 10.1186/s12970-017-0192-
[90] American Dietetic Association; Dietitians of Canada. (2003) ‘Position of the American Dietetic Association and Dietitians of Canada: Vegetarian diets.’ J Am Diet Assoc. 2003 Jun;103(6):748-65.
[91] European Food Safety Authority (2012) ‘EFSA assesses safety of long-chain omega-3 fatty acids’. https://www.efsa.europa.eu/en/press/news/120727. July 2012.
[92] British Dietetic Association (2019) ‘Iodine: Food Fact Sheet’. https://www.bda.uk.com/resource/iodine.html Accessed: May 2020
[93] Rogerson D. (2017) ‘Vegan diets: practical advice for athletes and exercisers.’ J Int Soc Sports Nutr. 2017; 14: 36. Published online 2017 Sep 13. doi: 10.1186/s12970-017-0192
[94] Van der Reijden O L, Zimmermann M B, Galetti V. (2017) ‘Iodine in dairy milk: Sources, concentrations and importance to human health.’ Best Practice & Research Clinical Endocrinology & Metabolism. 2017; 31(4)385-395.
[95] Bath, S., Button, S., & Rayman, M. (2012). ‘Iodine concentration of organic and conventional milk: Implications for iodine intake.’ British Journal of Nutrition, 107(7), 935-940. doi:10.1017/S0007114511003059
[96] British Dietetic Association (2019) ‘Iodine: Food Fact Sheet’. https://www.bda.uk.com/resource/iodine.html Accessed: May 2020
[97] Platel K, Srinivasan K. (2013) ‘Bioavailability of Micronutrients from Plant Foods: An Update.’ Crit Rev Food Sci Nutr. 2016 Jul 26;56(10):1608-19. doi: 10.1080/10408398.2013.781011.
[98] Rogerson D. (2017) ‘Vegan diets: practical advice for athletes and exercisers.’ J Int Soc Sports Nutr. 2017; 14: 36. Published online 2017 Sep 13. doi: 10.1186/s12970-017-0192
[99] Sebastiani G, Barbero A H, Borrás-Novell C, et al. (2019) ‘The Effects of Vegetarian and Vegan Diet during Pregnancy on the Health of Mothers and Offspring.’ Nutrients. 2019;11(3):557. Published 2019 Mar 6. doi:10.3390/nu11030557
[100] American Dietetic Association; Dietitians of Canada. (2003) ‘Position of the American Dietetic Association and Dietitians of Canada: Vegetarian diets.’ J Am Diet Assoc. 2003 Jun;103(6):748-65.
[101] Agnoli C, Baroni L, Bertini I, et al. (2017) ‘Position paper on vegetarian diets from the working group of the Italian Society of Human Nutrition.’ Nutr Metab Cardiovasc Dis. 2017 Dec;27(12):1037-1052. doi: 10.1016/j.numecd.2017.10.020. Epub 2017 Oct 31.
[102] American Dietetic Association; Dietitians of Canada. (2003) ‘Position of the American Dietetic Association and Dietitians of Canada: Vegetarian diets.’ J Am Diet Assoc. 2003 Jun;103(6):748-65.
Dining out of home and calorie-rich restaurant menus are often blamed as a main driver of the obesity issue worldwide. World Health Organization global estimates that more than 1.9 billion adults aged 18 years and older are overweight (WHO,2018). What if we could make healthier choices in restaurants more obvious and easier to make for consumers, with minimal effort on their part?
In a lot of cases, obesity is preventable. However, our current food environment makes this challenging. Behaviour change measures can be an effective means of changing consumer dietary habits. Consumer dietary choices are influenced by personal preferences, habits, nutrition information, availability, cost, and placement, among other reasons (Glanz & Bishop, 2010).
What can operators do to enhance positive, healthier behaviours in their establishments?
Research on behaviour change is showing the following 3 strategies are helpful tools to help encourage healthy behaviours. Read on for the ‘how’ behind these strategies.
- Ensure their menus provide visible and meaningful nutritional information to the consumer.
- Nutritionally optimise their recipes and provide healthier alternatives that motivate consumers to make healthier choices.
- Add environmental cues that encourage the healthy choice, such as signage at point-of-purchase, appealing pictures of healthy menu choices, etc.
What motivates us to make the choices we do?
Behaviour change can refer to a transformation or alteration of human behaviour or patterns. Approaches focusing on the individual, community and environmental influencers can support behaviour change.
Buying a car is one example. A person may be considering an energy efficient car as a more beneficial choice for the environment. Environmental influencers like awareness campaigns and financial incentives can motivate this individual’s purchase intent.
There are many credible models for behaviour change, one of which is the Capabilities, Opportunity, Motivation and Behaviour model (COM-B) of behaviour change.
Behaviour (B) occurs as the result of interaction between three necessary conditions:
- Capability (C): do you have the means available to do it? Money, time, or knowledge are examples.
- Opportunity (O): has the situation presented itself for you to make the change?
- Motivation (M): do you want to make the change?
Each of these conditions can influence each other, as well. The below figure shows there can be potential influences between components in the model; opportunity can influence motivation or capability. (Michie, Stralen & West, 2011).
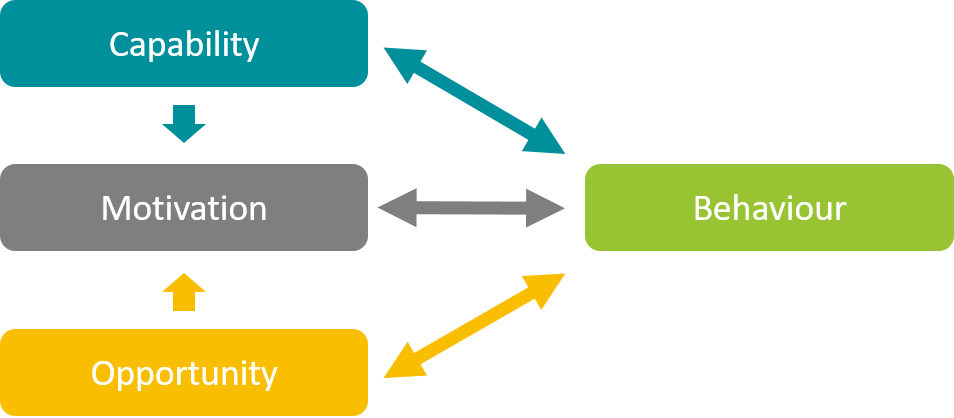
COM-B Model of Behaviour Change. Michie, Stralen and West (2011).
Applying this model to restaurants and away-from-home eating
Capability
is defined as the individual’s psychological and physical capacity to engage in the activity concerned. It includes having the necessary knowledge and skills. (Michie et al. 2011)

For example, the visibility of nutritional information can enable a consumer to make the healthier choice.
- Calorie labelling on menus when eating out of home,
- Front of pack labels such as the Keyhole logo used in the Nordic countries,
- Callouts of low-calorie options for example: “Under 600kcals”.
Calorie labelling on menus is an intervention that is being widely analysed and implemented in various countries such as USA, Australia and UK. A study by Bollinger et al, 2011 assessed the effectiveness of calorie labelling in 222 chain restaurants and found the labelling led to a 6% reduction in calories per transaction. Calories were posted on menu boards and menu in a font and format that was as prominent as the price. The reduction was a result of consumers changing their food choices, possibly due to the calorie information making them more capable to make the healthy choice.
The study also grouped consumers data into one of three categories of calories purchased: less than 125, between 125 and 250, or greater than 250 calories purchased. The data suggests that calorie labelling had a greater influence on consumers that tend to make high-calorie purchases with an average reduction of 26% calories per transaction.
A Cochrane review assessed the effectiveness of calorie labelling at point of consumption in restaurant settings. This intervention provided promising results that nutritional labelling on menus may reduce energy purchased. However, a wider set of measures would be recommended to tackle obesity (Crockett et al. 2018). Calorie labelling remains one tool in the toolbox to help tackle obesity.
Opportunity
is defined as all of the factors that lie outside the individual that make the behaviour possible or prompt it (Michie et al. 2011).
For example, the availability and accessibility of healthier products vs. unhealthier foods so that the consumer can easily make a healthier choice. If there are no healthy foods available when making a decision, there’s no opportunity to make the healthy choice.
Increasing availability of healthy foods was one of the top three interventions suggested in the McKinsey Global Institute report on Obesity (Dobbs et al, 2014). A review by Grech & Allman-Farinelli (2015) evaluated interventions in vending machines and found that sales of healthier items were increased when made available in five of the six identified studies, with no loss of overall sales volume. Increasing the amount of no added sugar beverages, low calorie snacks could change consumers purchase intent. In this example, people may have had sufficient capability to make the healthy choice but did not have the opportunity to do so until the healthy foods were added to vending machines.

Motivation
Capability and opportunity feed into motivation, which is defined as the brain processes that energize and direct behaviour, not just goals and conscious decision-making. It includes habitual processes, emotional responding, as well as analytical decision-making (Michie et al. 2011).
For example, promotional advertising of the healthier choices to entice and enthuse the consumer on digital platforms, social media or menu boards, or printed posters located near checkouts or within the consumers eye line can influence motivation by providing the right stimulus at the right time.
Advisory prompts through digital platforms or employees when a consumer selects their food of choice is another nudge tactic that can motivate healthier options (e.g. “would you like this without cream?”). A study focusing on the interaction between food choice and food advertisement exposure suggest that health-conscious consumers opted for the healthy snack following exposure to health message advertising (Dovey et al. 2017).
There are limited studies focusing on a combination of behaviour change interventions specific to dietary consumption when eating out of home. One pilot trial study involving 18 worksites in England evaluated three interventions assessing the impact on calories purchased. The interventions altered one of (a) portion size in six worksites (b) availability of healthier options in six worksites and (c) energy (calorie) labelling in six worksites.

The three intervention studies showed the following results
(a) Portion size – reducing portion sizes (by 10% or more) may be effective in reducing energy purchased and consumed from targeted food categories such as main meals, sides, desserts and cakes (Holland et al. 2018).
(b) Availability of healthier options, like offering more low-calorie options on a menu, could be a promising strategy to reduce calories purchased (Pechey et al. 2018). For example, lower calorie beverages or healthier side options incorporating fruit and vegetables or alternative cooking methods like baked vs. fried.
(c) Calorie Labelling – only one out of the six sites showed a reduction in calories purchased when calorie labelling was implemented in menus. However, the lack of a significant reduction in calories purchased in five out of the six worksites may have multiple explanations relating to barriers to calorie labelling implementation (Vasiljevic et al. 2018). The use of bigger fonts or differentiation through colour could highlight and make the calorie information more meaningful for consumers. In this case, enabling consumer capability by adding calories to menus may have not been enough to strongly motivate behaviour change.
The first two interventions, reducing portion sizes and increasing availability of healthier options, showed promising results for reducing calories purchased. These pilot study gives some positive indications that using these interventions in combination could promote healthier dietary patterns compared to using one of the strategies alone. However further research on a larger scale is needed to evaluate the optimal implementation and combination of these interventions.
Knowing is only part of the battle
Changing consumer behaviour takes time and can be very challenging, especially when eating out of home. Often, changes that do not require conscious decision making are the most effective. For example, reformulation to nutritionally optimise recipes is a method widely used by the food industry and recommended in many public health initiatives worldwide. It is an effective method of improving nutrition as it does not require any behavioural change from the consumer. Evidence is growing to suggest that changing small cues or slightly tweaking the physical environment may provide an effective way of changing behaviour, in ways that do not require a lot of cognitive processing by a consumer. These are commonly known as “nudge” interventions for example slight reduction in portions sizes or the placement of products near checkouts or on digital ordering systems to change the consumption behaviour of consumers (Vasiljevic, M et al. 2017).
Key takeaway
3 things operators do to enhance positive, healthy behaviours in their food environments:
- Ensure their menus provide visible and meaningful nutritional information to the consumer.
- Nutritionally optimise their recipes and provide healthier alternatives that motivate consumers to make healthier choices.
- Add environmental cues that encourage the healthy choice, such as signage at point-of-purchase, appealing pictures of healthy menu choices, etc.
Establishing a food environment that combines these approaches could potentially help shape the way in which food operators support consumers to promote healthier dietary behaviours.
Key takeaways from Pangborn 2019:
- Eating experience and environment has a large impact on food preference. Researchers and those seeking to maximize food preference need to consider consumer experience, using immersive techniques (e.g. augmented reality) to collect more realistic data.
- Sensory cues can be used to design products that can help make the healthy choice easier for consumers. For example, different textures can be used to help people feel more full when consuming smaller portions without compromising their taste experience.
Big data and the quest for new consumer insights to stay relevant
The theme of Pangborn 2019, a conference on sensory science and food preference held every 2 years, was ‘Engage with the future’. There was a broad acknowledgement among researchers and food industry leaders that the future is now, and for many this meant a move towards ‘big data’. Whether using social media and e-commerce sites to access ‘real-world’ consumer insights (e.g. A. Arellano-Covarrubias, Mexico), or adopting machine learning algorithms to enable big businesses to stay relevant by innovating earlier and faster (e.g. L. Depoortere, Belgium), methods to harness big data were at the top of the agenda. There was an important cautionary note to this trend, however, with others highlighting the inevitable trade-off between quality and quantity when acquiring these data, and urging businesses to consider how meaningful their big-data sensory and consumer insights truly are (e.g. T. Davis, UK).

Will augmented reality help place sensory and consumer science in context?
The relevance of traditional sensory and consumer methods and approaches was also a hot topic. The continued development and reformulation of food and beverage products is increasingly important, but optimising the impact of these products on health and wellness will require a much stronger integration with nutrition and psychological sciences. Despite clear sugar and calorie- reduction targets by governments world-wide, it was pointed out that we still do not know how best to label and present these reformulated products in a way that optimises consumer perceptions and behaviours (e.g. K. McCrickerd, Singapore). One problem is that traditional sensory and consumers approaches often fail to set the right context (a problem of ecological validity).
Whether consumption is at home (e.g. J. Delarue, France) or on the International Space Station (e.g. G. Douglas, USA) a consumer’s immediate environment, mood and motivations will impact how they perceive a food and the choices they make. Businesses are exploring Augmented Reality (AR) as a way to evoke realistic contexts during sensory and consumer testing and involve consumers in the co-creation of packaging design (e.g. L. Hewson, UK). While consumers appear to find this approach more engaging, realistic and enjoyable than traditional sensory and consumer tests, the true value-added from adopting this technology still remains to be seen.

A stronger focus on integrating Sensory, Nutrition and Health
A key message from the meeting was the link between sensory perception and health related behaviours. Food choices and intake decisions are informed by the sensory information perceived during consumption, and the taste, smell, and texture are important in guiding our eating behaviours. Several sessions at the Pangborn meeting focused on the impact of sensory cues on health, focusing on portion selection (e.g. M. Peng, New Zealand), texture cues and expected fullness (e.g. P. Varela, Norway) and new measures of oral processing behaviour (e.g. R. Srivastava, France).
The Kerry Health and Nutrition Institute co-organised a workshop entitled ‘Sensory Science as the Bridge between Consumer Behaviour, Nutrition and Health’ to highlight how sensory research is uniquely positioned at the nexus between food science, nutrition and consumer behaviour to better understand how perception can influence food intake, and be used to moderate the flow of energy and nutrients through our diets.
The workshop presented the latest findings at the interface of sensory and nutritional science, starting with a talk on the role of energy intake rate (kcals/min) in promoting calorie intake, and opportunities for sensory cues to support calorie reductions (C. Forde, Singapore). Prof Kees De Graaf from Wageningen University (Netherlands) highlighted some common mis-perceptions about the role of sweetness in dietary energy intakes, while Prof. Robin Dando (USA) shared exciting new findings that demonstrate the impact of increased weight gain on the development of taste buds, and the impact taste sensitivity changes can have on food choices. Finally, Dr. Nikos Pagidas from Kerry Taste and Nutrition highlighted a number of practical examples of sensory approaches to reformulating real products, while sustaining consumer appeal and satisfaction.
The meeting closed with the announcement that the next Pangborn meeting will be help in August 2021 in Vancouver, with the theme “Sustainable Sensory Science” – we look forward to seeing you there!
I often find myself wondering “what difference would personalized nutrition make?” Even if you could tell someone what food is healthy specifically for their genetics or lifestyle, so what? People have known for decades to eat more fruits and vegetables to improve their health, yet most people aren’t doing it. Scientists are debating every day whether the concept of personalized nutrition is even feasible.
Despite this, it almost seems like a topic that nobody can get away from. Media headlines are touting it as the future of nutrition and new start-up companies are creating products claiming to deliver nutrition personalized to measurements taken from blood or stool samples.
However, when I attended the American Society of Nutrition’s annual meeting for 2019 in Baltimore, a session about watermelon juice gave me a reminder: personalized nutrition is exciting, feasible, and it’s coming.
Personalized nutrition is exciting
What if I told you that you could improve your health by drinking watermelon juice every day, but if your friend drank the juice every day, they’d get no benefit?
Watermelons are rich in lycopene, an antioxidant possibly linked to heart health and other benefits. A recent study from the University of Alabama showed that watermelon juice was effective at raising lycopene levels in blood, meaning it could be beneficial for health.
In the study, the watermelon juice increased lycopene levels in blood by an average of 7.3 (µmol/L), but the reason personalized nutrition is exciting is what you see when you look at how each individual participant responded to the juice.
There was a wild variation in how well the watermelon juice actually increased lycopene levels in the blood for different particiapnts. For some people, the juice increased lycopene levels by 26 (µmol/L), but for other participants there was no effect at all. The researchers were able to attribute this to variations in genetics between each individual.
Personalized nutrition will help us make dietary recommendations more efficient for each person
Dietitians have been doing personalized nutrition for years: recommending dietary changes based on a specific person’s need states (e.g. heart health, exercise) and behaviors. For example, for heart health, a dietitian might recommend to increase intake of colorful vegetables, whole grains, and fiber, and this would most likely be effective at improving heart health measures.
But what if a dietitian could recommend foods to choose that were twice as effective for that individual’s specific genetics? Instead of ‘eat more fiber’, it’s ‘eat more barley’? This is the future you can see when you look at how different people’s bodies responded to the lycopene in the watermelon juice. You can make dietary recommendations, or tailored foods or beverages, much more effective without requiring any more work on the consumer’s part. It’s likely that someone knowing how effective a treatment will be will make them more likely to adopt and continue healthy behaviors.
It’s not here yet
Despite many companies and products claiming to deliver personalized nutrition solutions, science is still a long ways off from providing a true solution. Libraries will need to be built that link how different genes or microbiomes respond to different foods and nutrients. This is underway, and with fields like metabolomics becoming more efficient, it could come sooner than we think.
What sparked the conversation about personalised nutrition? To nutrition scientist Dr. Aoife Marie Murphy, two things stand out: the emergence of research on the gut microbiome alongside development of technology focused on tracking exercise and nutrition uniquely for each individual.
Aoife Marie Murphy, PhD, graduated with a BSc in Human Nutrition and a PhD in Nutrigenomics from University College Dublin. Her research interests include the dietary modulation of metabolic health, epidemiology and gene-nutrient interactions. She is currently a member of Kerry’s nutrition team where she helps apply research findings to innovative ideas in the food and beverage industry.
|
Get KHNI articles delivered to your inbox
|
Summary (scroll down for an infographic summary)
Topics & Speakers
Unlocking the Power of Phytochemicals – Beverages that Pack a Punch – Lisa Ryan, PhD, RNutr, Head of Department of Natural Sciences, GMIT
Identifying the Opportunities Behind Nutritional Beverages Using Sensory and Nutritional Sciences– Benedict Lawlor, PhD, Director of Sensory, Consumer & Analytical Sciences, Kerry
Nutrition science is making itself heard in the beverage category. Protein coffees, probiotic juices, and turmeric teas are common sightings as demand for convenient, functional foods increases with consumers. This leaves many of us asking the questions like:
“What is the future of nutrition for beverages?”, or “How can products continue to be differentiated?”
Watch this webinar to learn about:
- Emerging nutrition ingredients
- Improving satiety using sensory science
- Incorporating functional benefits
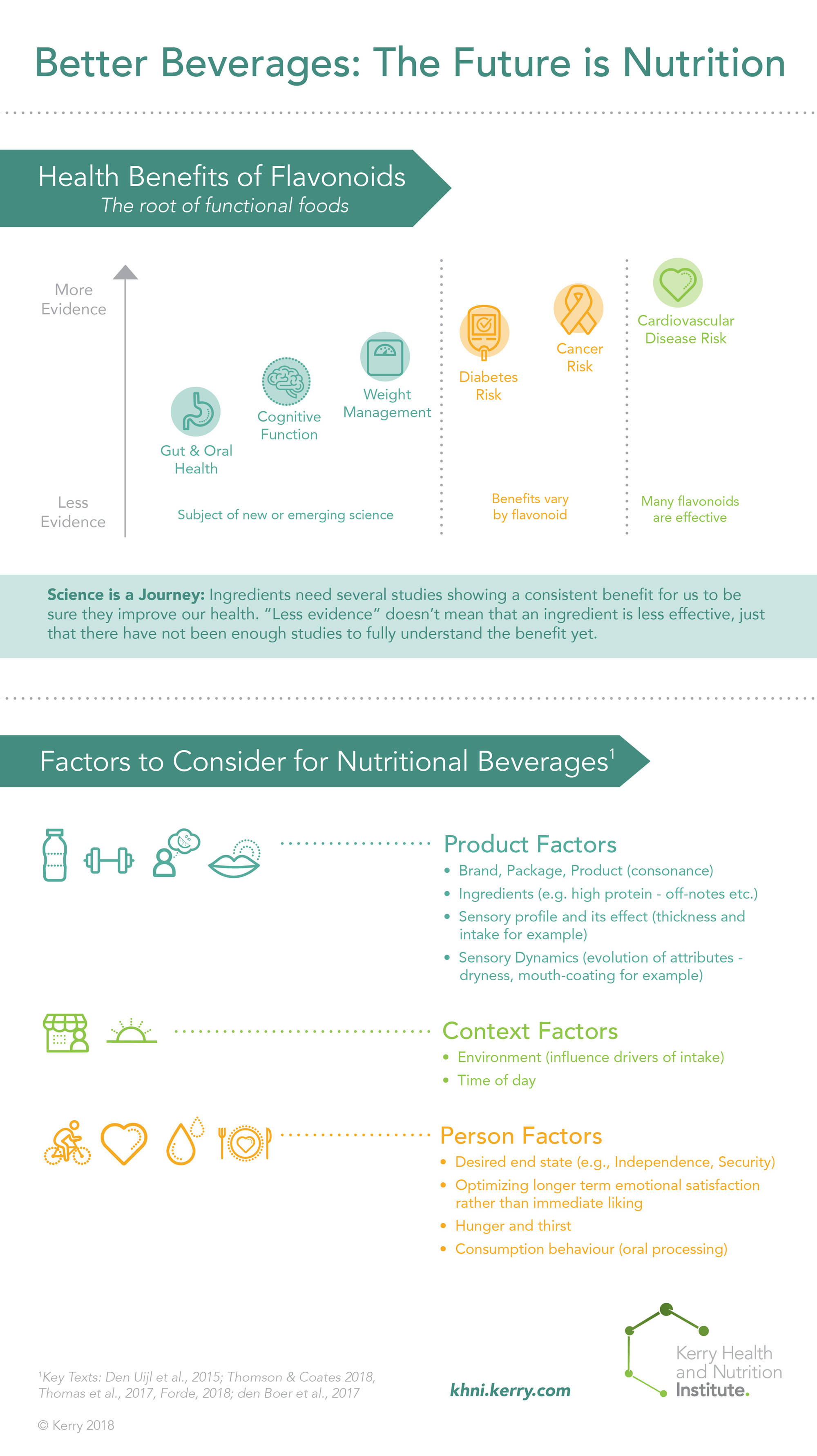
Personalized nutrition has been around for a long time, but technology has brought it mainstream
Dietitians have been doing personalized nutrition counseling for decades, but evolution of technologies and interest in food has brought personalized nutrition to the mainstream spotlight. This began with diet and activity trackers like MyFitnessPal, but has evolved to programs like DayTwo, which analyzes your gut microbiome to provide personalized nutrition recommendations. Companies like Habit hope take it a step farther by pairing nutrition advice that’s based on your own DNA with a meal delivery system, removing all of the guesswork. Drone delivery may bring another level of automation and convenience to the process, but what if we could even skip that step? What if we could print our own food that’s personalized to our needs at home? 3D printing has made its mark on many industries, and may be the future of personalized nutrition, as well.
What is 3D Printing?
Three-dimensional (3D) printing, also referred to as additive manufacturing, is a recently developed process in which materials are added layer by layer in a controlled, sequential manner using automated robotics to build up geometrically complex objects. 3D printing relies on an ink-like, flowable liquid or powdered material that can be quickly transformed into a rigid solid that serves as a foundation, or layer, that allows additional material to be ‘printed’ on top of this layer. The process is similar to the way frosting is piped, or extruded, from a piping bag onto a cake layer by layer to create intricate three-dimensional designs. 3D printing has been adapted to food materials, allowing modern chefs, food manufacturers, and do-it-yourself (DIY) innovators to produce novel food products with unique properties and shapes that cannot be replicated using traditional techniques of food design. For example, MIT’s Tangible Media Group has developed a 3D printed pasta that remains flat while dry but reacts with hot water to actively fold and form highly intricate shapes. And because 3D printing relies on software to direct the printing process, designs could be easily prototyped, saved, edited, and shared amongst collaborators across the world.
One of the earliest 3D printers used for food was the open-source Fab@Home Model 1 created by researchers at Cornell University in 2006. Chocolate was the first material adapted to food printing, as chocolate can be melted into an injectable form and quickly cooled to form a firm solid. Since then, many forms of the 3D food printer have been developed and adapted to several different food materials, including sugars, starches, cheese, meat, and gelatin. The primary limitation to 3D printing so far has been the restriction on the type of ingredients that can be readily liquefied or pulverized into a flowable form, and rapidly converted to a solid after extrusion.
In 2013, NASA contracted Systems and Materials Research Consultancy to explore the feasibility of 3D printing food in space for long-term missions. One of the parameters for the project was to investigate the nutritional quality of the foods generated using shelf-stable ingredients. The flavor and textural properties of the foods were studied to determine the acceptability of 3D printing for edibility and acceptability for human consumption. Overall, the goal of the project is to provide an alternative method to provide sustenance for space missions with greater variety and nutritional quality than the prepackaged foods that are currently used by NASA. This project has helped develop technology has since been used to start the company BeeHex, a start-up focused on developing 3D pizza printers for rapid personalized pizza production.

|
Get KHNI articles delivered to your inbox
|
Current Technology, Trends, and Challenges for Food Printing
3D food printing is still a nascent technology highly dependent on the advances made in 3D printing in general. Many 3D food printers are typically used for novelty purposes or DIY projects that are shared through not-for-profit open-source communities. Some 3D food printers are used by gourmet restaurants to prototype and create advanced culinary innovations. Currently there are few 3D food printers available for public use, and those on the commercial market are simple adaptations of multi-use 3D printers originally designed to print non-food materials, such as plastic, ceramic or metal. This is at least partly due to the high cost of purchasing and maintaining a 3D food printer, which can be prohibitive for home or commercial use.
Due to the small number of food ingredients suitable for generalized 3D printing, much of the innovation in the 3D food printing arena has been directed towards confectionary, bakery, dessert, and dough-based products for small-scale artisanal production. The materials used in these products (sugar, flour, chocolate, and egg) all possess the suitable properties outlined above, and can be readily joined together into solid shapes by applying simple precision heating using directed hot air or lasers. These ingredients can also be stored as shelf-stable powders that can form flowable inks by mixing with water or melting, which makes them readily adaptable to the 3D printing process. However, since it is difficult to create nutritious food from these ingredients, one of the main aims of the future of 3D food printing is expanding into key ingredients can be used to successfully create convenient, customizable and nutritious meals.
Some techniques have been developed and applied to 3D food printing to expand the available ingredients currently used. To print meat-based foods, a liquefied meat is extruded from the printer nozzle together with an enzyme called transglutaminase. The transglutaminase specifically acts on meat proteins and causes the liquid meat fluid to rapidly gel, forming a stable solid. Vegetables, fruits, and other high-water foods are liquefied and combined with a gel-forming ingredient, such as gelatin or agar, then cooled during printing to form solids. Some foods can be first printed in a semi-solid form and processed through cooking or drying to create a shelf-stable product, such as pasta.

Convergence of Nutrition and 3D Food Printing
While the technology has yet to be widely adopted, there are several ways in which 3D food printing could potentially impact the dietary and nutritional intake of consumers as the technology continues to grow. In most projected scenarios, consumers would own a 3D food printer as a household appliance that would allow them a high degree of customization during meal preparation. They would purchase pre-packaged food cartridge ‘inks’ containing various ingredients that could be mixed together in preprogrammed ways to create new ink formulations with tailored properties to be dispensed by the 3D food printer. Electronic recipe collections could also potentially be made available online that could be downloaded and used by the 3D printer to produce desired food products, similar to how documents can be shared online and readily printed on paper.
One example of the positive effect 3D printing can have on customer nutrition is giving consumers the ability to control the amount of nutrients in a product by manipulating the food ‘ink’ and automatically mixing various levels of nutrient ingredients into the ink in a predetermined way. Athletes who need precise nutritional profiles for the foods they eat to enhance performance could create or download programs for their 3D printer to prepare foods with exact concentrations of nutrients. The same method could be adapted to geriatric home or hospital care, in which each patient could have available food products designed specifically for their nutritional health needs. Similarly, parents with babies and young children who have strict dietary needs or restrictions could use the 3D printer to design nutritionally-enhanced and safe foods for their children.

Furthermore, consumers could combine different food inks to enhance the sensory appeal of their meals in ways unavailable with current home meal preparation techniques. By combining predesigned flavor ink cartridges with bulk food ingredients, a fully customized set of flavored foods could be produced by the 3D printer appliance. The same principle could be applied with colored inks as well as texture-enhancing ingredients. Due to the layer-by-layer nature of 3D printing, consumers could create flavor, color and texture gradients with incredible aesthetic and artistic appeal. With the ability to customize and combine nutrition with desirable sensory properties, a 3D food printer could allow householders to enhance the taste of their foods while simultaneously introducing high-nutrient ingredients beneficial for health.
Conclusion
The ability to create custom flavor and color gradients combined with formulating precise mouthfeel, shapes, and nutritional content could expand the possibility for household meal preparers, patient care institutions, schools, athletes, and other health-conscious consumers to create foods with tailored qualities attractive to different demographics. While 3D food printing is still yet to be widely available to the public at an affordable price tag with broad functionality, continued breakthroughs in this technological space will hopefully yield a powerful tool for food creation and personalized nutrition in the future.
In a study published in the journal Rheumatology, researchers examined the role between nutrition and osteoarthritis. Osteoarthritis is a condition driven by inflammation, resulting in joint pain. It is one of the fastest growing causes of disability worldwide. Here’s what the researchers found to be effective at reducing osteoarthritis symptoms.

Fish oil
Omega-3 fatty acids from fish oil were the main nutrient shown to reduce joint pain in the study. An added benefit was improvement of cardiovascular health markers in these individuals. The study showed that individuals who were able to reduce raised cholesterol levels also had reduced symptoms, so it’s possible the fish oil was acting in both ways to improve outcomes.
Vitamin K
Vitamin K is needed to help create proteins important for bone and cartilage health. Results from the study suggest increasing intake of vitamin-K rich foods, like leafy greens, may have helped alleviate symptoms in study participants.
Weight
Overweight and obesity are the main contributors to development of osteoarthritis due to the mechanical stress the extra weight places on joints. Reducing weight, combined with exercise tailored to mobility, was the number one recommendation to come from the study.
Although not included in the study above, anti-inflammatory compounds like curcumin have also been shown in some studies to alleviate symptoms of osteoarthritis. Expect to see more products combining traditional nutrition, via vitamins and minerals, with bioactive compounds, like curcumin, as demand for functional food continues to rise.
For the full study details, click here.
Related
Summary (scroll down for an infographic summary)
Speakers
Sugar Reduction Around the World – Consumer, Health & Legislation Demands: Aisling Aherne, PhD, RNutr, Nutrition Science Manager, Kerry
Overcoming the Complexities of Reduced Sugar: Ashley Baker, VP RD&A, Kerry

In a world that loves sugar’s familiar qualities…where do you start for its successful reduction?
Sugar ranks at the top of the list when it comes to consumer nutrition concerns, but sugar reduction poses a challenge across all product categories. The responsibility and cost of helping consumers reduce their sugar intake is being pushed onto the food and beverage industry by legislation like sugar taxes.
We look at why so many sugar-reduced products fail. Though consumers cite taste as the biggest driver of their intention to repurchase, we explore other key factors that may stop great-tasting products from getting off the shelf.
Hear from nutrition and applications experts on how to succeed with sugar reduction. Find out what makes healthier products likeable while fitting into labelling and tax legislation across the world. Bringing together consumer perception research, true nutrition science and practical formulation expertise, you’ll come away with actionable insights, practical examples and industry-relevant solutions for sugar reduction.

Trends in the food and beverage industry are moving more and more toward the idea of ‘natural’, including eating less processed food. This can leave many of us wondering ‘what is the role of processed food for my nutrition?’

A scientific statement in the American Journal of Clinical Nutrition titled Processed foods: contributions to nutrition dug into the data to see if processed foods help us meet dietary guidelines, or provide a hurdle.
What the authors found was that processed foods are critical in helping most of the population meet their nutrient requirements. Specifically, processed foods provided an average of:
- 55% of fiber intake in the US
- 48% of calcium
- 43% of potassium
- 34% of vitamin D
- 64% of iron
- 65% of folate
- 46% of vitamin B12
Many of these have been called out as nutrients to consume more of in diets and deficiency of them is linked with conditions like anemia (iron, B12), osteoporosis (vitamin D, calcium), or birth defects (folate).
Although processed foods are helping many people meet their recommended nutrient intakes, these foods are often higher in nutrients we should limit in our diets than less processed foods. The data shows that processed foods account for:
- 57% of our daily calorie intake
- 52% of saturated fat
- 57% of sodium
- 75% of added sugar
This means there are clear opportunities to reduce content of these nutrients to limit in the diet, especially added sugar and sodium.
What does ‘processed’ really mean?
The word ‘processed’ has wildly different definitions depending on who is using it. To many consumers, it can mean foods on the perimeter of the grocery store. More formal definitions of processing include the following examples, and can be done in the household setting or in a factory.

Heating, freezing, canning, fermenting, drying, smoking, peeling, milling, extrusion, etc
By these definitions, many healthy foods would be considered processed, like oatmeal, frozen vegetables, fermented foods like yogurt, and more.
Due to the variation in types of processing, many organizations have tried to provide a formal definition. The study in the AJCN used the definitions from the International Food Information Council to separate foods by the degree to which they’re processed. The 4 categories are minimally processed foods (washed fruits or vegetables), foods processed for preservation (canned tuna), ready-to-eat foods (breakfast cereal), foods processed for safety or visual appeal (spice mixes), and foods packaged to stay fresh and save time (prepared deli foods).
Ideals vs Reality
Despite the strong push to avoid processed foods in many trendy diets, the study shows the bulk of what we eat is processed in some way. Although eating a diet of only minimally processed foods could sound like a healthy choice, the reality is many people don’t have the access to these types of foods (e.g. food deserts), time or skills to prepare them, or money to afford them. Most likely, processed foods are not going anywhere any time soon, but we can focus on making these foods more similar to minimally processed foods. The ability to create processed foods that are convenient while also providing important nutrients will be key for future innovations. At the same time, sugar and sodium must continue to be reduced to keep consumers within healthy calorie limits. Innovations that help reduce these nutrients while maintaining flavor and functionality will be key for the future, as well.
Could fat be the key to maintaining flavor when modifying sugar or salt levels in food? A new study in the journal Food Quality and Preference explores the impact fat content has on liking of soups and custards with varying levels of fat, sugar, and salt content.

Researchers provided study participants either creamy tomato soup or custard in four fat concentrations (0, 7.5, 15, or 30% fat), combined with four salt concentrations in the soup (0.04, 0.35, 0.7, or 1.5%), and four sugar concentrations in the custard (0.56, 4.5, 9, 18%). The goal was to determine the extent to which fat content impacted perception of salt or sweet flavors, as well as overall liking.
When it came to salt, the relationship was simple: fat and salt independently affected how much participants enjoyed the soup. In other words, more salt=tasty, and more fat=tasty. The relationship was more complicated for sugar in the custard, though. Although fat and sugar both impacted how much participants enjoyed the custard, there was also an interaction between the two nutrients that affected how pleasant the custard tasted. This could mean that more sugar+more fat=tastier than having more of either alone.
The study findings have interesting implications for the food and beverage industry. The researchers noted that sugar and salt both had stronger impact on liking of the foods than fat content. However, with the strong drive to reduce sugar and salt across product categories, keeping fat at reasonable levels in products could help solve some of the taste challenges that come with reduction of these nutrients.
Sugar taxes have seen news coverage in recent years as a way to decrease sugar intake, but a new study found potential merit for additional price changes to improve health.

A study from Tufts University published in BMC Medicine found that changing the price on 7 foods by 10% could prevent an estimated 23,000 deaths per year from cardiometabolic disease.
The study moved beyond the idea of taxing nutrients we should get less of, like sugar, to include the idea of subsidizing healthy foods like fruit, vegetables, whole grains, and nuts. The study also included a tax on processed and unprocessed red meats.
This research suggests taxes on unhealthy foods and subsidies for healthy foods may reduce deaths from stroke, diabetes and cardiovascular disease, especially among Americans with lower socioeconomic status.
Sugar taxes have been controversial in legislation, but research shows it is likely achieving its intended purpose. Taxing and subsidizing the bulk of the food supply would likely be quite complicated in practice, but this research shows it’s not something that should be ruled out just yet.
Summary (scroll down for an infographic summary)
Speakers
What’s Driving the Clean Label Movement? Practical Insights – Joseph Borchardt, Strategic Marketing Director, Kerry
Nutrition & Healthy Food: Behind the Label – Nathan Pratt, PhD, RD, RD&A Scientist, Nutrition, Kerry
 Healthy eating has never been more talked about, and the ‘free-from’ trend has been dominating the consumer marketplace. Consumers are increasingly demanding foods that are free from allergens like gluten or dairy, artificial ingredients like flavors and preservatives, and any ingredients with unfamiliar names. The response of the food industry to this booming consumer demand is a ‘Clean Label’ movement. Food and beverage manufacturers in every category and channel are innovating and evolving to stay ahead of these changing consumer needs by reducing the number of ingredients on labels, removing unfamiliar ingredients, and building trust with consumers.
Healthy eating has never been more talked about, and the ‘free-from’ trend has been dominating the consumer marketplace. Consumers are increasingly demanding foods that are free from allergens like gluten or dairy, artificial ingredients like flavors and preservatives, and any ingredients with unfamiliar names. The response of the food industry to this booming consumer demand is a ‘Clean Label’ movement. Food and beverage manufacturers in every category and channel are innovating and evolving to stay ahead of these changing consumer needs by reducing the number of ingredients on labels, removing unfamiliar ingredients, and building trust with consumers.
To consumers, though, it is about more than a clean ingredient label. Kerry has undertaken proprietary research to gain insight into what consumers want from their food and its labelling. Where do these fit into market trends? How do these expectations impact food and beverage manufacturers? We found that consumers are looking past “marketing speak” for foods that fit an expanded definition of healthy, for food they can trust, and food closer to nature.
Join us for a webinar which looks to the future of healthy eating and the impact on the food industry. See why cleaner labels may just be part of a solution for an expanded consumer definition of health, and why nutrition, social and environmental responsibility will be key to successfully meet long-term consumer needs for healthy food.
|
Get KHNI articles delivered to your inbox
|
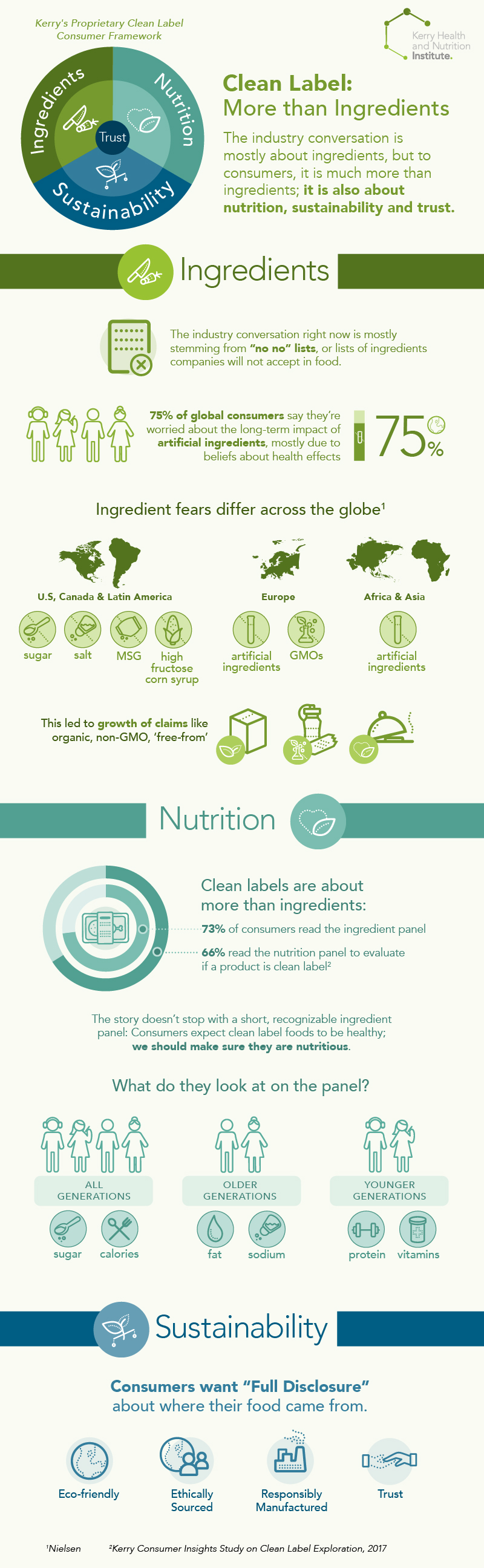
A new study found that many medical students lack the knowledge to properly counsel patients on nutrition, yet still feel confident to provide recommendations to patients. This is a concerning combination, since primary care physicians are a main source of health-related information for much of the population.

Specifically, the study found only 12% of students were aware of the Dietary Reference Intakes, which are the most current recommendations for nutrient needs based on factors like sex, age, etc. The second year students in the study scored an average of 74.2% on a quiz designed to test nutrition knowledge, yet 68% of the students felt that nutrition counseling was the responsibility of the primary care provider (PCP).
Few students in the study could accurately define the role of Registered Dietitians in patient care, despite RDs being the key resource for medical nutrition therapy for patients.
“The member of the health care team most proficient in medical nutrition therapy or nutrition education and counseling is the registered dietitian (RD) or registered dietitian nutritionist (RDN). Ideally, physicians would refer patients in need of nutrition counseling to RDs/RDNs. However, most patients are not referred because of countless physician barriers, including time, lack of insurance coverage, finances, and confidence in a patient’s willingness to change behaviors. For this reason, primary care physicians (PCPs) are often the sole source of nutrition education or nutrition counseling”
Although this study was only limited to one medical program, the disconnect between the importance placed on nutrition by study participants and their knowledge gaps means medical training and testing procedures may need to evolve to help fill student needs. The study authors recommend including nutrition knowledge on board certification exams and requiring physicians to shadow RDs/RDNs to better understand their role in the patient care process as potential solutions.

The most cutting edge nutrition and food science research around the globe is conducted in university laboratories, but did you ever wonder what happens to this research once it’s published in a journal? Who uses it? Does it just collect dust? How do the benefits shown in the research make it to consumers?
Or do you wonder how food and beverage companies decide what nutrients to put into products? Is science even involved in the process?
Hear straight from university and industry researchers about the benefits of partnership for advancing science and health in this video.
Partnerships between university researchers and scientists in the food and beverage industry are essential to drive innovation. For the industry, this partnership provides new insights into good science coming down the pipeline, identifies new ingredients to put into food that delivers health benefits to consumers, and can help frame an innovation pipeline spanning multiple years. For university researchers, the partnership provides the opportunity to bring their research to life in real products that reach consumers.
Do vegans have healthier eating and health behaviors than omnivores? A recent study in the journal Appetite found that health behaviors don’t differ much between them.

People who choose to be vegans (not consume any animal products) could choose to do so for reasons ranging from ethical to health-related. However, there isn’t much research to show if people who choose to be vegan are actually healthier than omnivores.
In the study, researchers looked at eating and health behaviors of 358 vegans and compared them to those of 220 omnivores. They found vegans were more likely to consider themselves healthy, prepare food at home, and consume healthy foods like fruits, vegetables, and beans more often than omnivores. However, the researchers noted that these differences were small and found no significant differences in BMI between the groups.
What does this mean for someone debating becoming vegan? It’s probably not necessary if your only goal is to be healthier. Many of the differences found in the study could be due to vegans generally paying more attention to their diet than the omnivores of the study, rather than specifically avoiding animal products. It’s probably much easier for most people to have a healthy, balanced diet as an omnivore than by restricting intake of a large number of food groups. Read our blog Tipping the Balance Toward Moderation for more on keeping a healthy, balanced lifestyle.
Sensory science could be seen as a traditional way to validate the sensory aspects of a food, or it could be seen as a way to strategically link nutrition to food choice. Ciaran Forde, PhD, a researcher in the area of sensory science and food choice, discusses why he thinks sensory science is evolving to become the bridge between nutrition and behavior in this video.
Ciaran Forde, PhD is a Principal Investigator of Human Nutritional Sensory Science at the Singapore Institute for Clinical Sciences.
Joanne Slavin, PhD, RD is a leading nutrition researcher in the areas of fiber and general wellness. We sat down with her to get her perspective on the future of nutrition, including hot topics like plant proteins, changing fiber regulations, and what’s on the horizon.
Dr. Slavin is a Professor in the Department of Food Science and Human Nutrition at the University of Minnesota and a member of our Scientific Advisory Council.
The Role of Flavors in Nutrition
With busy lifestyles, many consumers are relying on the food industry for convenient and affordable sources for meals. There is a big emphasis not only on the cost and nutritional value of these options, but also on the taste and eating experience from the purchased items. Flavors play an essential role in enhancing the taste experience. This experience, which includes aspects like flavor, aroma, and mouthfeel, becomes more important in the case of healthy food options where fat, sugar, salt and calories reduction are emphasized. Flavors are extremely essential in rebalancing the taste profiles associated with removal of excess fat, sugar, salt. For example, a reduced fat ranch dressing may be improved with the addition of dairy flavors that would give the perception of creaminess that is reduced when the actual fat component is lowered. In diet sodas, the replacement of sugar with a high-intensity sweetener usually results in off-tastes of the sweetener, i.e. bitter/ metallic notes, lingering sweetness and loss of mouthfeel.

These off-notes can be reduced and improved upon with the addition of flavors. Nutritionally enriched food items such as meal replacement/nutrition beverages or bars fortified with high amounts of protein, vitamins and minerals come with a lot of taste challenges. Proteins often have strong flavors that can create off-notes, or can interact with vitamin and minerals and create flavors frequently described as bitter, beany, metallic and chalky. Flavor solutions can help reduce the off-note perception of the nutritional enrichment. In short, flavors are very much an essential tool for the food manufacturer in the pursuit of introducing healthier, cost-effective and also good-tasting food options to the consumer.
Natural Flavors
Currently, the trend for natural flavors has been on the rise due to the consumer’s desire for wholesome and minimally processed foods. With the advent of food bloggers such as the Food Babe and also natural and organic food movements, there has been an even bigger momentum for food manufacturers to move away from artificial additives in food and replace them with natural ingredients, such as natural flavors, in their food. The definition of healthy is expanding to include foods without additives and with easy-to-read ingredients, similar to a food that was home-cooked. Common requests from consumers include: does not contain artificial flavors, colors or preservatives, GMO-free, and free from pesticides and hormones.

However, unlike the label ‘organic’, which has a fixed set of rules and regulations in order to receive the correct labelling status, the label ‘natural’ in the US is not regulated. Natural flavors can be briefly described as an extract derived from foods (plant, animal, spice etc.) or from a ‘natural’ process such as fermentation and enzymatic conversion. The Flavor & Extracts Manufacturers Association (FEMA) provides additional description of natural flavors here.
In the EU, there are more specific regulations and guidelines for the labelling of natural flavors. Flavorings can be labelled with the term “natural” only if their flavoring part consist of entirely “natural flavoring substances” and/or “flavoring preparations”. The definitions of these natural flavoring components include the source materials they are obtained from and the processes they are obtained by. The specific descriptions of natural flavorings labelling would depend on what is present in the flavoring part and the flavor perception how they were made i.e. natural flavoring, natural flavoring substances, natural (example) raspberry flavoring and natural (example) strawberry flavoring with other natural flavorings. For a named natural flavor, for example natural orange flavoring, at least 95% (by weight) of the flavor must originate from orange and the flavor perception of the named source needs to be easily recognized. For the other type of natural flavor label, e.g. ‘natural orange with other natural flavorings’, flavoring components derived from orange are present and their flavor can easily be recognized. For the other ‘natural flavorings’ in this label, the flavors can be derived from different source materials other than orange.
|
Get KHNI articles delivered to your inbox
|
Challenges with Natural Flavors

The use and sourcing of natural flavors are not without its challenges. Natural flavors are usually more expensive to manufacture and also not as potent as their synthetic counterparts. For example, a vanilla extract made from the extraction process of vanilla beans costs significantly more than synthetic vanillin. Because natural flavors are not usually as potent as synthetic, a higher dosage of flavor will have to be used which would increase cost in use (CIU) in the final product. There are also problems associated with obtaining raw materials for natural flavor extraction. For example, vanilla crop yield is very susceptible to poor weather conditions and also unstable political/ humanitarian situations and citrus based flavors which have been severely impacted in the past decade and a half by the greening disease. The greening disease is caused by the bacterium Candidatus Liberibacter asiaticus which results in diseased, unhealthy trees with small, dark green fruit with bitter tasting juice. There is no cure for this disease except by the burning of the infected trees to prevent further transmission of the bacterium and this has severely reduced and affected citrus production in the USA, Brazil, Asia and other part of the world.
The Future of Natural Flavors
There have been many groups advocating for a formal regulatory process to obtain the ‘natural’ labelling status for foods and flavors, as is seen in the case of ‘organic’ labelling which has very strict and defined guidelines. In the US, the FDA is in the process of evaluating the status of the ‘natural’ label. With an even stronger demand by consumers for foods which are free of additives, preservatives and flavors (both natural and unnatural), there might be a push to even remove the label ‘flavor’ entirely from processed foods. This would pose definite challenges on food processors to deliver good tasting foods without flavors. Labelling of the flavors might also be changed, e.g. in a cheese flavor, it would not be declared as a flavor but as cheese, water and enzymes instead. There might be more of a push from the food industry to modify the way a food is processed and the base ingredients used to maximize flavor development of a product instead of topical application of a flavor. For example, slow roasting of a food to develop complex savory flavors. This would lead to higher costs of the final product which the consumer must be willing to bear in exchange for removing items like natural flavors from food labels.